 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
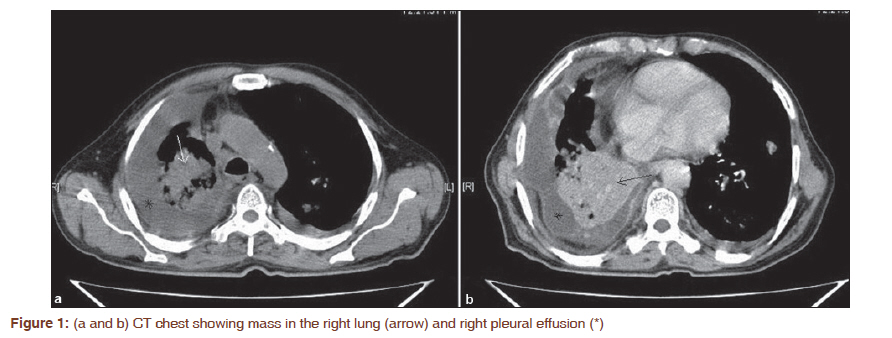
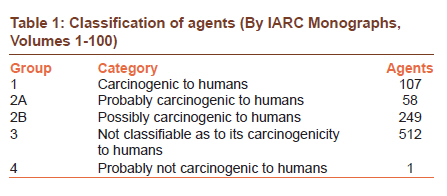
Journal of Cancer Research and Therapeutics, Vol. 7, No. 3, July-September, 2011, pp. 358-360 Letter to the Editor - Documenting a Case Adenocarcinoma lung in a painter Arinaganhalli Subbanna Praveen Kumar, Ramalingam Chandramohan, Dharanitragada Krishna Suri Subrahmanyam, Tarun Kumar Dutta Department of Medicine, Jawaharlal Institute of Postgraduate Medical Education and Research, Pondicherry, India PMID: 22044826 DOI: 10.4103/0973-1482.87012 Lung cancer is one of the leading causes of cancer deaths worldwide. More than 1.1 million cases of lung cancer are diagnosed annually, and over 1 million deaths are caused by the disease. [1] The most important risk factor is tobacco smoking. Several agents encountered in the occupational setting, such as asbestos, polycyclic aromatic hydrocarbons, arsenic, beryllium, cadmium, chromium, and nickel compounds, are established carcinogens that target the lung. Many cohort and linkage studies of painters have shown consistent and significant increases in lung cancer compared with the general population (IARC monograph volume 98, 2010). The principle pigment used in paints is white pigment titanium dioxide (TiO 2 ). The IARC categorized TiO 2 as potentially carcinogenic to humans (group 2B). Although occupational exposure to TiO 2 is extensive, there are few data on the levels and sources of exposure. [2] There is an evidence of carcinogenicity in experimental animals for TiO 2 but the evidence in humans is sparse and equivocal. A 40-year-old male painter by occupation for the past 25 years presented with 2 months history of cough, breathlessness and right lateral chest pain. There was no history of fever, haemoptysis or contact with tuberculosis. He is not a smoker or alcoholic and there was no history of other comorbid illness. The general physical examination revealed pulse rate of 90/ min, blood pressure of 130/80 mmHg, pallor and there was no lymph node enlargement. Respiratory system examination revealed diminished breath sounds and dull percussion note in the right axillary, right infrascapular area and there were no added sounds. Abdominal examination showed hepatomegaly and other system examination were normal. Laboratory examination revealed normal liver and renal function tests. The peripheral smear showed haemoglobin 9 mg/dl, total count of 6000/ dl with normocytic normochromic blood picture. The human immunodeficiency virus test (HIV), hepatitis B surface antigen (HbsAg), antibodies to hepatitis C virus (anti-HCV) was negative. The chest X-ray showed right massive pleural effusion. CT chest revealed mass in the right middle and apical lobe with right pleural effusion [Figure - 1]a and b and ultrasonography abdomen showed multiple nodular lesions in the liver suggestive of liver metastases. The pleural fluid showed elevated protein (6 mg/dl) and cytology of pleural fluid was suggestive of adenocarcinoma. The lung biopsy was not done as patient refused to give consent. Paint is a suspension of finely divided pigment particles in a liquid composed of a binder and a volatile solvent or water. The most common pigment employed in paint is the white pigment TiO 2 , produced from ilmenite ore or from titanium slag. TiO 2 was first produced commercially in 1923, primarily for pigment production. It is primarily used as whitening and mollifying agent in paints, varnishes, lacquers, paper, plastics, ceramics, rubber and printing ink. [3] TiO 2 is generally present in paints in proportions varying between 10% and 20% and probably below 2 mg/cubic mm during most spray paint operations. [2] The spray painting in closed spaces without protection can lead to the inhalation of high concentrations of TiO 2 . The IARC conducts evaluations of carcinogenic risks of different agents, and thereby provides the information base for cancer prevention throughout the world [Table - 1]. [4] According to IARC (monograph volume 98, 2010) report, occupational exposure as a painter is carcinogenic to humans (Group 1). Humans are exposed to TiO 2 via inhalation, ingestion or dermal contact. It has been shown in experimental rats, that long-term inhalational exposure to carbon black, TiO 2 and talc to produce pulmonary inflammation, fibrosis and lung tumors. [4] The respiratory effects observed among groups of TiO 2 -exposed workers include decline in lung function, pleural disease with plaques and pleural thickening and mild fibrotic changes (IARC monograph, volume 93). There have been three large cohort studies [5],[6],[7] among production workers in the TiO 2 industry. The largest, conducted in six European countries, found a slightly increased risk for lung cancer compared to the general population. [5] However, there was no evidence of an exposure response relationship within the cohort. The other cohort studies, [6],[7] both of which were conducted in the USA, did not report any increased risk for lung cancer. The recent study conducted in Montreal showed that people exposed to TiO 2 did not experience any excess risk of lung cancer. [8] The results of the study by Siemiatycki et al. showed possible increase in lung cancer risk among subjects with high exposure to TiO 2 . [9] The cytogenetic studies on painters reported increased levels of genetic damage, such as chromosomal aberrations, micronucleus formation, sister chromatid exchange [10] and single strand DNA breaks. Our patient occupation was painting mainly interior painting, spray painting and primer paintings of wooden blocks and metals for more than 20 years. The predominant pigment involved in most paints was TiO 2 . He used to work predominantly in closed spaces without proper facemask and more importantly he is not a smoker. Since there was prolonged exposure to paint for more than 20 years without proper protection, this would have been predisposed him to develop lung adenocarcinoma. He presented to us in the terminal stage of lung carcinoma with metastasis to the liver. He was planned on palliative chemotherapy after medical oncology consultation but he did not give consent for further management and discharged from hospital against medical advice. In conclusion, painters are at risk of developing lung carcinoma on prolonged exposure and hence a proper precaution has to be taken at working place. And also whether TiO 2 is carcinogen to the lung in humans or not is still unanswered question. More case series studies and case reports may aid in this regard. References
Copyright 2011 - Journal of Cancer Research and Therapeutics The following images related to this document are available:Photo images[cr11090t1.jpg] [cr11090f1.jpg] |
| |||||||||

{kind=link}
{kind=link}