 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
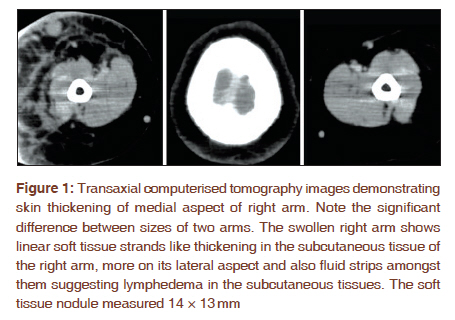
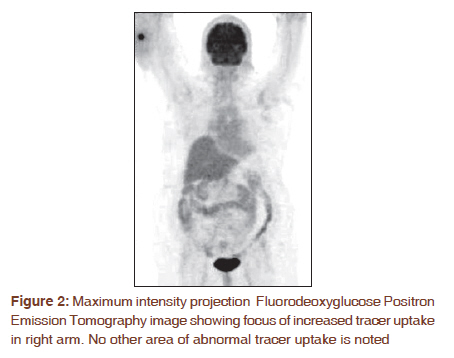
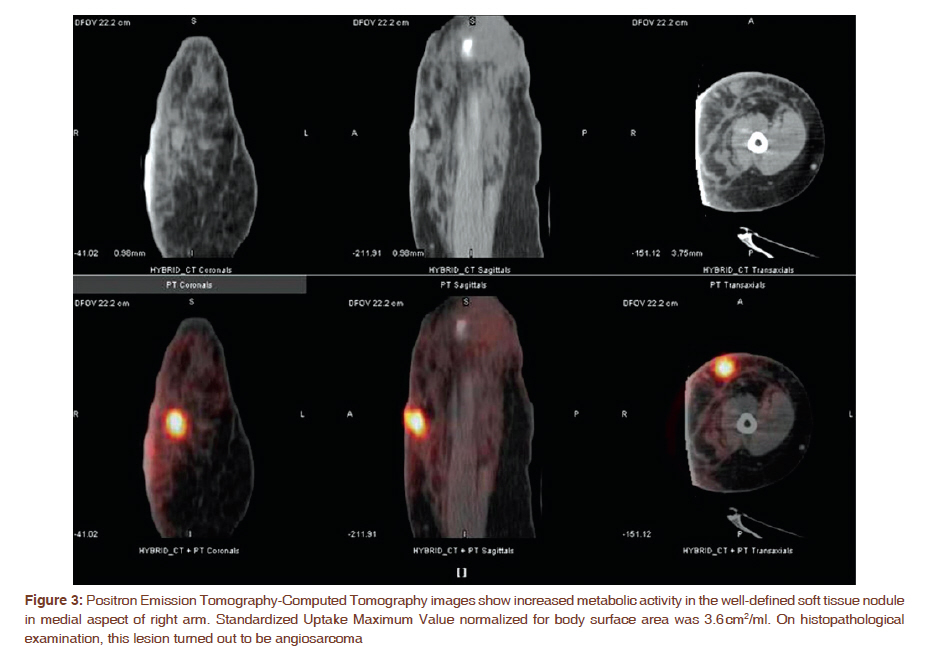
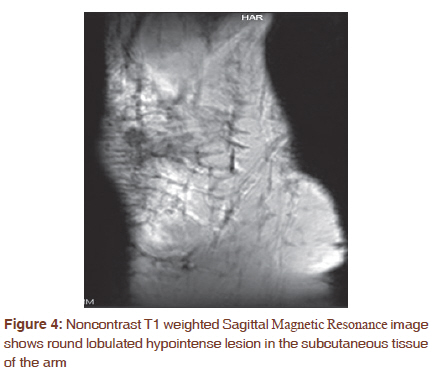
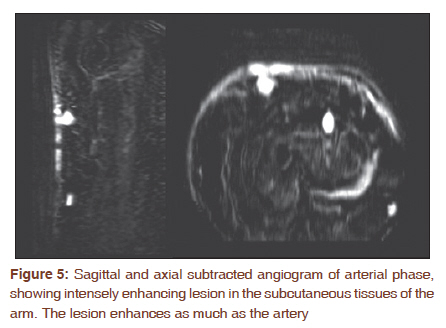
Journal of Cancer Research and Therapeutics, Vol. 7, No. 3, July-September, 2011, pp. 360-363 Letter to the Editor - Documenting a Case Fluorodeoxyglucose positron emission tomography-computed tomography scan and nuclear magnetic resonance findings in a case of Stewart-Treves syndrome Prathamesh Joshi1, Vikram Lele1, Rozil Gandhi2 1 Department of Nuclear Medicine and PET-CT, Jaslok Hospital and Research Centre, Mumbai, India PMID: 22044827 DOI: 10.4103/0973-1482.87014 Stewart-Treves syndrome is a cutaneous angiosarcoma that develops in long-standing chronic lymphedema. This tumor develops as a very rare complication in patients suffering from chronic lymphedema of the upper limb following mastectomy and axillary lymph node dissection for breast cancer. [1] We present FDG PET-CT and NMR imaging characteristics of this rare complication of lymphedema. A seventy year old lady, known case of carcinoma right breast, presented with nodular erythematous lesion over right arm. Her treatment history included right modified radical mastectomy (MRM), with axillary lymph node dissection followed by local radiotherapy seven years ago. Post-surgery she developed lymphoedema of right arm. FDG PET-CT was advised to characterize the right arm lesion and to evaluate the whole body disease status. Transaxial CT images [Figure - 1] demonstrate skin thickening of medial aspect of right arm. The swollen right arm shows linear soft tissue strands like thickening in the subcutaneous tissue of the right arm, more on its lateral aspect and also fluid strips amongst them. These findings suggest lymphedema in the subcutaneous tissues. The soft tissue nodule measured 14 × 13 mm. FDG PET-CT images [Figure - 2] and [Figure - 3] show increased metabolic activity in the well-defined soft tissue nodule in medial aspect of right arm. Standardized Uptake Maximum Value (SUVmax) normalized for body surface area was 3.6 cm2/ml. These findings were highly suggestive of neoplastic etiology. NMR was also performed in this patient to know the exact soft tissue extent of the PET-CT demonstrated lesion. Noncontrast T1 weighted Sagittal NMR images [Figure - 4] showed round lobulated hypointense lesion in the subcutaneous tissue of the right arm. Sagittal and axial subtracted angiogram of arterial phase [Figure - 5] demonstrated intensely enhancing lesion in the subcutaneous tissues of the arm. On biopsy, the lesion was found to be angiosarcoma. Considering the history of chronic lymphedema following breast surgery, a diagnosis of Stewart-Treves syndrome was made.We present the FDG PET-CT and NMR findings in this rare syndrome. The Stewart-Treves Syndrome is an angiosarcoma, appearing in a specific clinical setting. The diagnosis relies on medical history, clinical examination and a histological assessment. [1] In 1948, Stewart and Treves reported this rare secondary malignancy in 6 cases of angiosarcoma in post-mastectomy lymphedema. They recognized that long-standing chronic edema without recurrent cancer may occasionally produce "a heretofore unrecognized and unreported sequel, long after the malignant breast neoplasm has apparently been arrested a new specific tumor". [2] Most common interval between radical mastectomy and the onset of lymphangiosarcoma was 5-14 years. [3] Our patient has history of chronic lymphedema (7 years) after modified radical mastectomy with axillary lymph node dissection and local radiotherapy for treatment of right breast carcinoma. The typical history, NMR and FDG PET-CT findings were suggestive of neoplastic etiology, the lesion turned out to be angiosarcoma on biopsy. Positron emission tomography is known to improve pre-operative staging in patients with sarcoma. [4] More recently PET CT scans have been demonstrated as having higher sensitivity, specificity and accuracy than PET or CT alone. [5] Use of FDG PET-CT in cases of angiosarcoma in the setting of lymphedema has been described in the past. [6],[7] It has been proposed as important tool in staging and treatment planning of STS. [7] NMR is the examination of choice for local staging of both bone and soft tissue tumors including sarcomas. [8] Combination of contrast and non-contrast NMR gives useful information. Contrast increases signal intensity of tumors on T1 images and may enhance demarcation between tumor and surrounding soft tissue, on the other hand distinction between tumor and adjacent muscle is usually well demarcated on non-contrast scans. [9] Unfortunately, for patients with angiosarcoma the prognosis is poor. A large surgical resection is the treatment of choice if the patient is a candidate for a surgical resection with a curative intent Radiotherapy is sometimes used as a palliative local treatment. Chemotherapy is only used in more advanced cases, not curable by surgery alone. [1] To conclude, our case demonstrates FDG PET-CT and NMR appearance of Stewart- Treves Syndrome. In our case, FDG PET CT not only helped in the characterization of primary lesion but also evaluated the whole body status. Even though rare, this diagnosis must be kept in mind while evaluating lesions in extremities in patients with chronic lymphedema. References
Copyright 2011 - Journal of Cancer Research and Therapeutics The following images related to this document are available:Photo images[cr11091f5.jpg] [cr11091f2.jpg] [cr11091f4.jpg] [cr11091f3.jpg] [cr11091f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}