 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
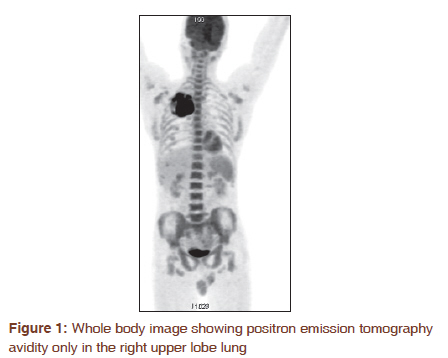
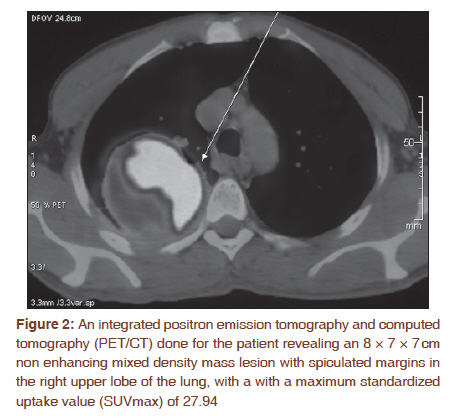
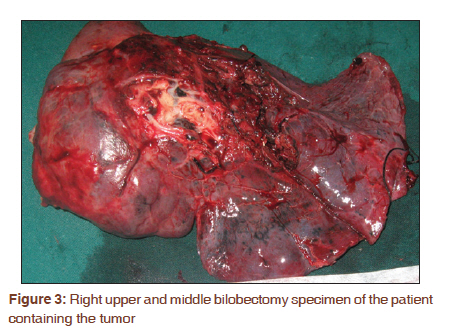
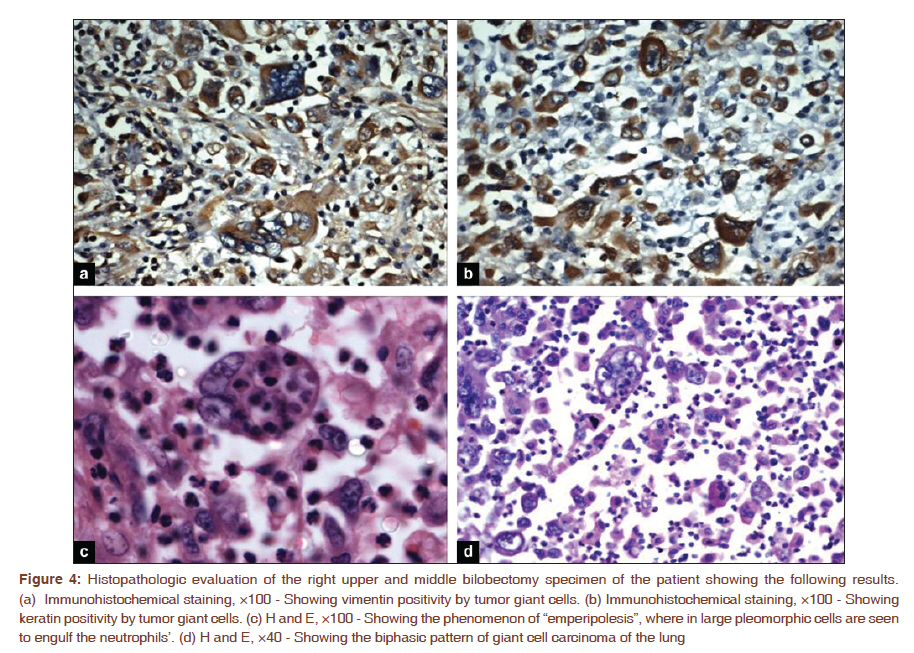
Journal of Cancer Research and Therapeutics, Vol. 7, No. 3, July-September, 2011, pp. 363-365 Letter to the Editor - Documenting a Case A fatal case of pure giant cell carcinoma of the lung Arvind Krishnamurthy1, N Vijayalakshmi2, Urmila Majhi3 1 Department of Surgical Oncology, Cancer Institute (WIA), 36, Sardar Patel Road, Adyar, Chennai - 600 020, India Lung cancers are an extremely heterogeneous family of malignant neoplasms′, with well over 50 different histological variants recognized under the 2004 revision of the World Health Organization (WHO) classification. [1] GCCL, a rare histological type of non small cell lung cancer (NSCLC), is now classified as one of the five subtypes of sarcomatoid carcinoma of the lung. We recently treated a 56 year old gentleman with this aggressive subtype and describe our experience. A 56 year old gentleman, a former smoker (40 packs/ year), with no co morbid illnesses′, presented to his family physician with a history of cough and hemoptysis of 2 months duration. He was evaluated there with a chest skiagram and a computerized tomography (CT) chest which showed right upper lobe opacity. On further evaluation at our center, we found his general examination to be unremarkable, physical examination revealed decreased air entry in the right lung apex. An integrated positron emission tomography and computed tomography (PET/ CT) done subsequently revealed an 8 × 7 × 7 cm non enhancing mixed density mass lesion with spiculated margins in the right upper lobe of the lung with a maximum standardized uptake value (SUVmax) of 27.94 [Figure - 1] and [Figure - 2]. A CT scan guided aspiration cytology from the right upper lobe mass lesion was not contributory and so were the bronchoscopic brushings and lavage cytologies. His echocardiogram and pulmonary function tests were within normal limits. He was taken up for a right thoracotomy and underwent an uneventful right upper and middle bi-lobectomy with mediastinal lymph node dissection after a frozen section confirmation of malignancy [Figure - 3]. Histopathology revealed a poorly differentiated high grade malignant tumor with extensive necrosis and vascular invasion. The tumor showed bilobar and parietal pleural involvement and reactive adenopathy in eleven mediastinal nodes. The tumor on microscopy showed sheets of mononuclear and multinucleated atypical giant cells in an inflammatory background. The mononuclear cells were large polygonal to fusiform with pleomorphic vesicular nuclei and prominent nucleoli and moderate eosinophilic cytoplasm. The multinucleated cells were bizarre with 2-6 nuclear lobes with marked cellular and nuclear pleomorphism and coarse chromatin. The phenomenon of "emperipolesis", where in large pleomorphic cells are seen to engulf the neutrophils, was demonstrated. The immunohistochemical profile was positive for Epithelial Membrane Antigen (EMA), keratin, vimentin, Leucocyte Common Antigen (LCA) and Neuron Specific Enolase ( NSE). The final impression was that of a pure GCCL [Figure - 4]a-d. The patient was pathologically staged as pT3N0M0 and was considered for adjuvant chemotherapy with cisplatin and etoposide. However after the third cycle, the patient was increasingly symptomatic for shortness of breath, and on evaluation with a CT scan was found to have a pleural thickening with a moderate hemorrhagic effusion, whose cytology was twice negative for malignancy. The patient declined further intervention and wished to be on best supportive care. His general condition rapidly deteriorated and he succumbed to his disease nine months post surgery. GCCL, a rare histological type of NSCLC, was first described by Nash and Stout in 1958. [2] It was initially classified as a type of pleomorphic carcinoma (PC). Prior to 1999, PC was considered a variant of other well-known NSCLCs; however, its diagnosis was problematic in view of a lack of uniform diagnostic criteria. In 1999, the World Health Organization (WHO) re-classified PC to include spindle cell carcinomas combined with squamous cell carcinoma, adenocarcinoma, giant-cell carcinoma, or large-cell carcinoma based on light microscopic findings, sometimes supported by immunohistochemistry. However, in the WHO 2004 classification, GCCL were classified as a subtype of sarcomatoid carcinomas of the lung. Five subgroups of sarcomatoid carcinomas representing a pathological-morphologic continuum are currently recognized: PC, spindle-cell carcinoma, GCCL, carcinosarcoma, and pulmonary blastoma. [1] The typing of these tumors thus has been a subject of controversy and confusion over the years. The reported incidence of pure GCCL is 0.1%-0.4% of all lung cancers. The characteristic giant cells in GCCL have been described as pleomorphic and anaplastic, with both mononuclear and multinuclear forms. [3] This classical biphasic pattern makes pre operative cytological diagnosis very difficult. The final diagnosis in most instances is made on the histological analysis of the resected specimen or in some cases on autopsy. Another feature that makes this malignancy unique is the presence of the phenomenon of emperipolesis. [2] This feature is commonly seen in megakaryocytes in the setting of thrombocytosis, regardless of etiology. The etiology of emperipolesis in the setting of GCCL is obscure. As in our case, the literature shows GCCL to have a male preponderance, more so among smokers. The other epidemiological and clinical features seem similar to that of other NSCLC s . [4] In a clinic pathologic study of 78 cases of PC of the lung, 65% of the tumors were located in the upper lobes and 47% of which were in the right upper lobes, [4] as also seen in our patient. The therapeutic strategies adopted for GCCL are the same as for patients with other variants of NSCLC, however the prognosis for the former is worse [4],[5],[6] GCCL has been regarded as an aggressive cancer with more than half of the cases presenting with metastatic disease and median survivals being in the range of 8-10 months. However, a few case series has shown a better prognosis with surgical resection of early stage disease. [4],[5],[6],[7] Little information is available on systemic treatment options for this tumor. Traditionally, standard platinum-based therapeutic approaches similar to that used in NSCLC have been used in such patients, although with poor response rates. [8],[9],[10] Radiotherapy has also not proven to be an effective modality for this variant of lung cancer. Clinicians involved in the management of lung cancer should be aware of this rare but aggressive histological variant of NSCLC. Clearly, further studies are needed to better understand the biology of this tumor, so as to identify novel therapeutic targets aiming at improving the final outcome. References
Copyright 2011 - Journal of Cancer Research and Therapeutics The following images related to this document are available:Photo images[cr11092f4.jpg] [cr11092f1.jpg] [cr11092f3.jpg] [cr11092f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}