 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
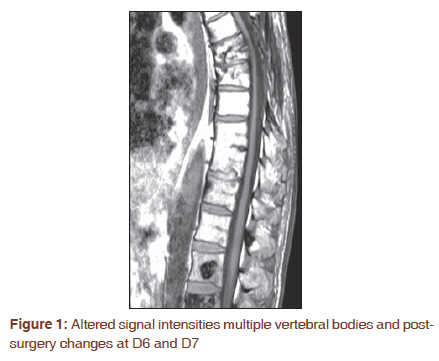
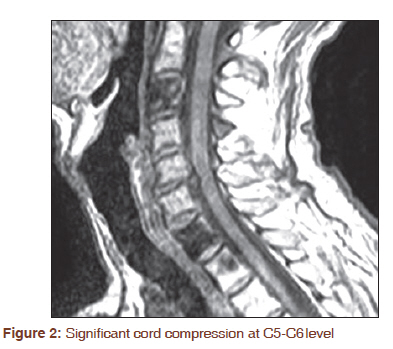
Journal of Cancer Research and Therapeutics, Vol. 7, No. 3, July-September, 2011, pp. 366-367 Letter to the Editor - Documenting a Case Oncological progression of bone plasmacytoma to POEMS syndrome Narendra Kumar Rathore, Ajay Sharma, Shyama Prasanna Sathpathy, Rahul Walke Department of Radiotherapy, Acharya Tulsi Regional Cancer Research and Treatment Centre, SP Medical College, Bikaner, Rajasthan, India POEMS syndrome is defined by the presence of polyneuropathy (P), organomegaly (O), endocrinopathy (E), monoclonal gammopathy (M), skin changes (S), papilledema, edema, pleural effusion, ascites and thrombocytosis. Virtually all patients will have either at least one bone lesion or coexistent Castelmans disease. All features of the disease are not required to make the diagnosis. The peak incidence of POEMS syndrome is in the 5 th and 6 th decades. It is frequently confused with chronic inflammatory demyelinating polyneuropathies. The mainstay of therapy includes irradiation, corticosteroids, alkylators-based therapy and high-dose chemotherapy with peripheral blood stem cell transplantation We describe a case of POEMS syndrome that first presented as vertebral plasmocytoma and than progressed to POEMS syndrome after asymptomatic period of 8 years. A 59-year-old male patient was presented with history of lower limb paresis. MRI showed architectural disruption of D6 vertebra with soft tissue component and epidural cord compression. Laminectomy was performed. Morphology of tumor tissue was suggestive of plasma cell tumor. Bone marrow biopsy and aspirations were negative. Sign and symptoms of end organ damage were absent. Rest of routine investigation was normal including calcium, hemogram, 24-hour urine for Bence-jone protein, renal and liver function tests. One month later, adjuvant external radiotherapy was delivered as single fraction of 8 Gray followed by ten fractions of 3 Gray and eight cycles of adjuvant chemotherapy were delivered using vincristine, adriamycin and dexamethasone. Patient was remain asymptomatic for 8 years than presented with lower limbs weakness with difficulty in walking and numbness in all limbs. Neurological examination revealed bilateral motor paresis in lower limbs and glove-stocking type of anesthesia in all limbs. Routine investigations showed moderate hepatomegaly with fatty changes, mild cardiomegaly and abnormal raised random blood sugar. MRI showed altered signal intensities in approximately all vertebral bodies predominantly in D1 and D2, post surgery changes at D6 and D7 [Figure - 1] and spondolytic protrusions at C5-C6 level causing significant cord compression [Figure - 2]. Cervicomedullary junction was normal and no adjacent soft tissue component was found. Endocrinal evaluation revealed diabetes mellitus type-2. The bone marrow biopsy and aspiration were negative for plasma cells. Twenty-four-hour urine test was negative for Bence-Jones protein. The monoclonal M-protein was detected only on immunofixation and was not evident on electrophoresis. Skin changes, ascites and effusion were not appeared. POEMS syndrome is a chronic progressive polyneuropathy with a predominant motor disability. The acronym POEMS (polyneuropathy, organomegaly, endocrinopathy, M protein, and skin changes) refers to several dominant features of the syndrome; however, there are associated features not included in the acronym including sclerotic bone lesions, Castleman disease, papilledema, thrombocytosis, peripheral edema, ascites, effusions, polycythemia, fatigue and clubbing. [1],[2],[3] To make the diagnosis, a patient should have the following: the peripheral neuropathy, osteosclerotic myeloma (i.e., clonal plasma cell dyscrasia and at least one sclerotic bone lesion) or Castleman disease and at least one of the other features. [3] Though the majority of patients have osteosclerotic myeloma, these same patients usually have only 5% bone marrow plasma cells or less, and rarely have hypercalcemia or renal insufficiency. These characteristics and the superior median survival differentiate POEMS syndrome from multiple myeloma. Our patient presented mainly with symptoms of polyneuropathy, motor weakness and endocrinopathy with previous history of plasmocytoma. While multiple myeloma is usually characterised by the development of lytic bone lesions, there have been rare cases associated with widespread osteosclerotic lesions. [4] In our patient, distinction from multiple myeloma is based on the absence of dispersed plasma cells on bone marrow biopsy and aspiration, absence of Bence-Jones protein in urine and absence of related organ impairment. It is interesting to note that the monoclonal M-protein was detected only on immunofixation and was not evident on electrophoresis. This is a recognized phenomenon that is reflective of the low magnitude of the protein spike in POEMS and should be borne in mind when investigating clinically suspected cases. [3] The plasma cells are virtually always λ-restricted. Although the pathophysiological mechanism is not well understood, there is a correlation between treating the underlying plasmaproliferative disorder (clone) and clinical improvement. Radiation therapy produces substantial improvement of the neuropathy in more than half of the patients who have a single lesion or multiple lesions in a limited area. If there are widespread lesions, conventional chemotherapy or high-dose chemotherapy and peripheral blood support may be helpful. The overall median survival of patients with POEMS was 13.7 years in a large series. Those with clubbing or extravascular volume overload had median survivals of 2.6 and 6.6 years, respectively. [3] Patients with POEMS syndrome have limited response to plasmapharesis and intravenous immunoglobulin therapy. [5] Those with single or multiple osteosclerotic lesions in a limited area are usually treated with radiation and more than 50% of patients will have some response. [3] Some patients with solitary osteosclerotic lesions respond to surgical excision. [5] There have been reports of patients responding to excision of larger lesions even in the presence of more diffused lesions with marked improvement in polyneuropathy. [6] In those who have not responded, high-dose chemotherapy and peripheral blood stem cell transplant have been suggested. [3] These options should be considered in patients who do not respond to standard therapy. This case also illustrates the importance of immunofixation in detecting low levels of monoclonal protein when investigating a demyelinating polyneuropathy, the need for close monitoring, re-evaluation and consideration of aggressive surgical therapy and high-dose chemotherapy with stem cell support in patients with POEMS who do not respond to initial treatment. References
Copyright 2011 - Journal of Cancer Research and Therapeutics The following images related to this document are available:Photo images[cr11093f1.jpg] [cr11093f2.jpg] |
| |||||||||

{kind=link}
{kind=link}