 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
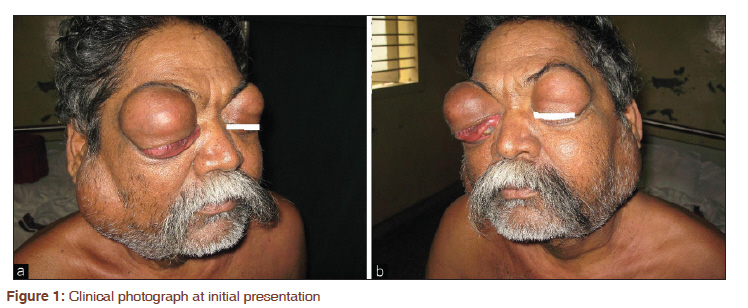
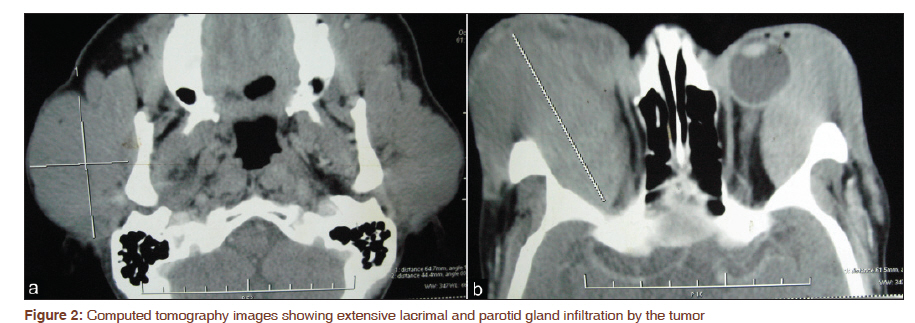
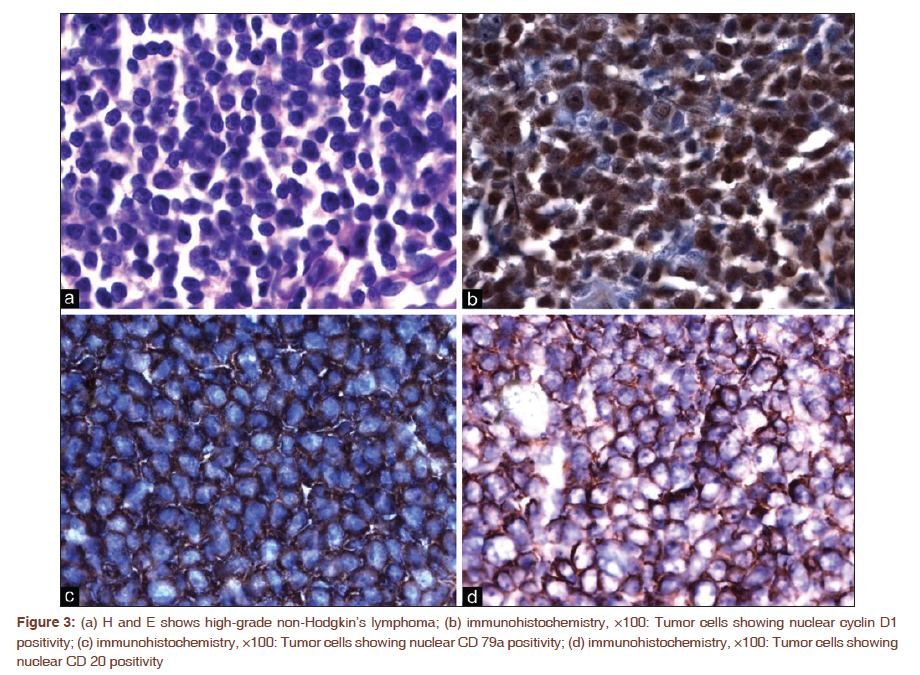
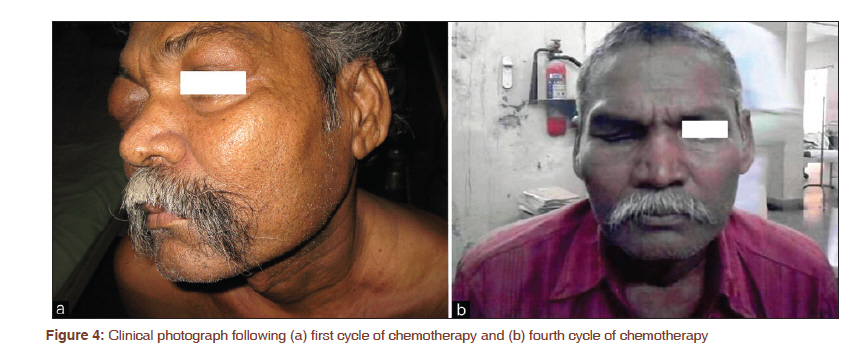
Journal of Cancer Research and Therapeutics, Vol. 7, No. 3, July-September, 2011, pp. 372-375 Letter to the Editor - Documenting a Case Mantle cell lymphoma presenting as Mikulicz syndrome Arvind Krishnamurthy1, Akash Shah2, Prashanth Ganesan2, TG Sagar2 1 Department of Surgical Oncology, Cancer Institute (WIA), Adayar, Chennai - 600 020, India Johann Von Mikulicz-Redecki, a student of Theodore Billroth, published in 1892 a case report of a middle-aged farmer with bilateral enlargement of the lacrimal and salivary glands. Mikulicz himself concluded that the nature of the disease was a mystery. There has been a great deal of confusion with regard to the description of Mikulicz disease and Mikulicz syndrome (MS) ever since. The former is described to be an idiopathic disease, while the latter is described to be a symptom complex caused by a variety of benign and malignant disorders. We present an interesting case of mantle cell lymphoma (MCL) presenting with initial presenting features attributed to MS. A 54-year-old man presented to us with insidious onset of progressively enlarging swellings of both the upper eyelids, parotid, and upper neck of 1 year duration. The patient first noticed the swelling in both his upper eyelids, which began to grow to an extent that opening the eyes and formally accessing visual acuity became difficult. There was no perception of light in his right eye, in the left eye, however, there was perception of light and he could appreciate finger counting from a distance of 4 m. The enlargement of both the parotid glands appeared a few months after the lacrimal gland swelling and it interfered with his mouth opening and eating. He had no constitutional symptoms; his past medical history was insignificant. Clinical evaluation revealed significant painless enlargement of both the lacrimal, parotid, and submandibular glands [Figure - 1]. The right lacrimal gland swelling measured 7 × 5 cm, while the left measured 6 × 4 cm, and the right parotid measured 9 × 9 cm, while the left measured 9 × 8 cm. The measurements of the right and left submandibular glands were 6 × 6 cm and 6 × 5 cm, respectively. All the swellings were painless, well circumscribed, soft to firm in consistency (the right lacrimal gland swelling was firm to hard because of fibrosis) with normal overlying skin. There was no organomegaly or lymphadenopathy. The clinical examination of the cardiovascular, respiratory, gastrointestinal, and the neurologic systems were unremarkable. His hemogram and biochemical investigations were within normal limits and so were his bone marrow aspiration and biopsy. A computed tomography (CT) scan of the head and neck revealed the enlarged salivary and lacrimal glands [Figure - 2]; there was insignificant bilateral cervical lymphadenopathy, and the CT scan of the chest and abdomen was normal. A tru-cut biopsy from the right parotid gland swelling was done to establish a tissue diagnosis. The microscopy revealed a tumor composed of sheets of round to oval cells with scanty cytoplasm and vesicular nuclei and smaller nucleoli, scattered lymphoepithelial inclusions were also seen, the impression favored a non-Hodgkin′s lymphoma (NHL). The immunohistochemistry profile showed strong positivity for LCA, CD5, CD20, Cd79a, Bcl2, and cyclin D1. The smaller lymphoid cells were positive for UCHL1 and CD23. CD10 was negative, while Bcl6 was inconclusive. The final impression was that of an NHL stage II E (extranodal) mantle cell lymphoma [Figure - 3]a-d. He was planned for chemotherapy with cyclophosphamide, vincristine, doxorubicin, and prednisolone (CHOP). There was a dramatic response with near complete disappearance of all the swellings except the right lacrimal gland swelling starting just after the first cycle of chemotherapy [Figure - 4]a. The visual acuity in his left eye was recorded at 6/6 (20/20 feet) on the Snellen chart, however, the visual acuity in his right eye was beyond 6/60 (20/200 feet), probably due to extensive lymphomatous involvement. He has successfully completed 4 cycles of CHOP [Figure - 4]b and is continuing his chemotherapy protocol. The diagnosis of Mikulicz disease is based on the following criteria: (a) persistent (>3 months), symmetrical swelling of the lacrimal and major salivary glands; (b) prominent mononuclear cell infiltration of lacrimal and salivary glands; and (c) exclusion of other diseases presenting as glandular swellings. [1] MS on the other hand is a symptom complex caused by a variety of systemic disorders both benign and malignant with secondary involvement of the lacrimal and salivary glands. The malignancies associated with MS include rare case reports of NHL, Hodgkin′s lymphoma, leukemia, and lymphosarcoma. [2] Some authors, however, feel that there is too much confusion surrounding the terms Mikulicz disease and MS, they critically evaluated the elegantly written 1892 publication by Mikulicz himself and concluded that the riddle of the nature of the disease was solved, it being a MALT lymphoma. [3] Recent studies have suggested that the lymphoid hyperplasia of IgG4-related systemic disease (including Mikulicz disease) could provide a possible substrate for the emergence of lymphomas. Cheuk et al. [4] reported 3 cases of ocular adnexal lymphomas arising in IgG4-related chronic sclerosing dacryoadenitis along with 3 other cases of ocular adnexal extranodal marginal zone B-cell lymphoma that showed sclerosing inflammation in the background and numerous IgG4+ monotypic plasma cells; however, such an association was not reported by Plaza et al., in their retrospective review of orbital biopsy specimens of patients with orbital manifestation of IgG4 associated systemic disease. [5] MCL is a distinct clinical entity constituting 3%-10% of the NHL, being listed as a peripheral B cell lymphoma. [6] It is a neoplasm of the monomorphous small- to medium-sized B cells with irregular nuclei and a characteristic translocation t(11; 14) (q13; 32), resulting in overexpression of cell cycle protein cyclin D1. [6],[7] It has a male preponderance and is commonly seen in the middle-aged to older men. The clinical presentation often includes extranodal involvement, particularly of the bone marrow and gut. [6] Although the involvement of either of the salivary and lacrimal glands as part of generalized lymphomas has been described, the presentation of lymphomas as MS is a rare occurrence. Being accepted as a separate clinical entity for only the last two decades, the number of clinical trials for MCL is not extensive as for some other varieties of NHL. The optimal management of these patients is not known, options range from wait and watch [8] to aggressive multiagent chemotherapy and autologous transplant. [9] The most commonly used chemotherapeutic schedules include a combination chemotherapeutic regimens consisting of varying combinations of cyclophosphamide, vincristine, doxorubicin, and prednisolone with or without rituximab. MCL is generally considered to be an aggressive disease and none of the biologic and clinical prognostic factors has been validated as a tool for the selection of therapy, it is therefore recommended to start therapy at diagnosis while tailoring treatment to the age and the general condition of the patient. [10] Given the overall poor prognosis, patients are encouraged to participate in clinical trials with newer agents in order to determine the optimal chemotherapeutic regimen. In conclusion, a differential diagnosis of lymphoma is to be considered in any patient presenting with features suggestive of MS so as to ensure prompt initiation of appropriate treatment. References
Copyright 2011 - Journal of Cancer Research and Therapeutics The following images related to this document are available:Photo images[cr11095f1.jpg] [cr11095f4.jpg] [cr11095f3.jpg] [cr11095f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}