 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
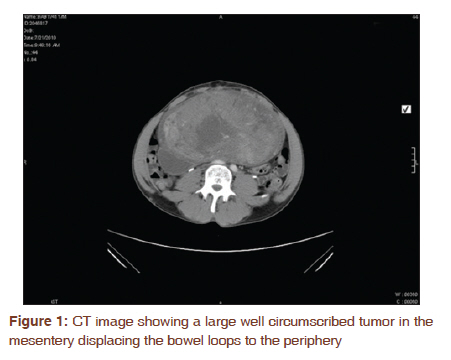
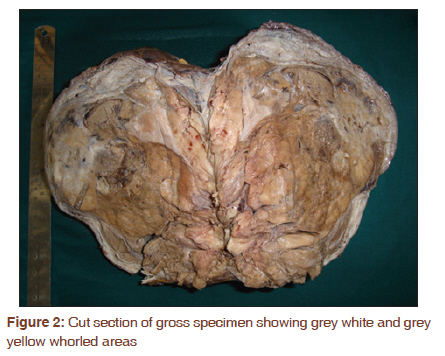
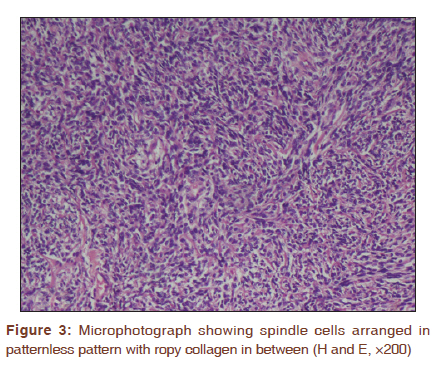
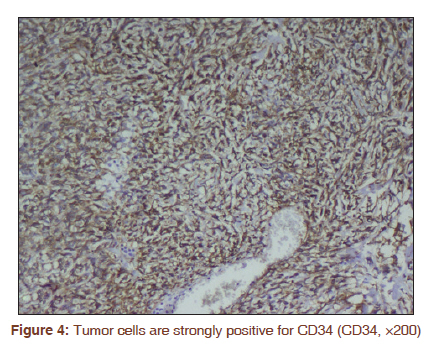
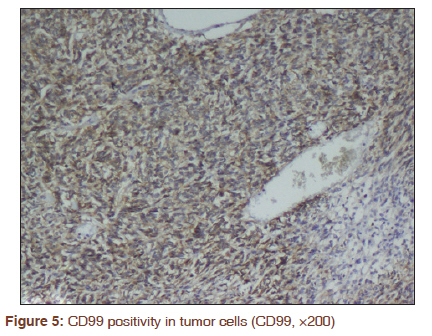
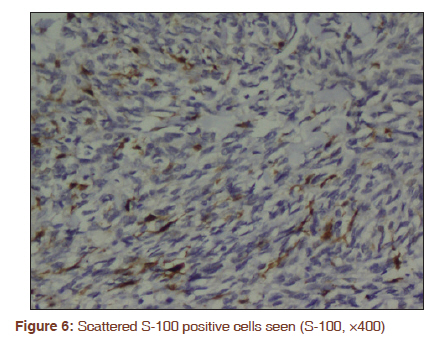
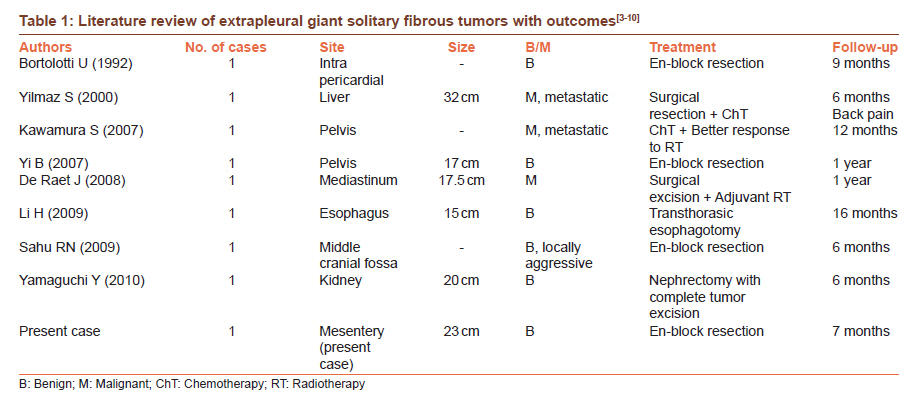
Journal of Cancer Research and Therapeutics, Vol. 7, No. 3, July-September, 2011, pp. 376-378 Letter to the Editor - Documenting a Case Giant solitary fibrous tumor of the mesentery: A rare case Ranjini Kudva1, Vidya Monappa1, Anand Rao2 1 Department of Pathology, Kasturba Medical College and Hospital, Manipal University, Manipal, Karnataka, India Solitary fibrous tumors (SFTs) are uncommon tumors principally arising in the pleura and have also been reported to arise from various extra-pleural sites. On rare occasions, they can assume large sizes (up to or >30 cm) when they are called as GSFTs. Review of the literature for tumors diagnosed as GSFT revealed less than 25 cases, out of which only 8 cases were from extra-pleural sites. To the best of our knowledge, this is the first case of GSFT arising in the mesentery. In this report, we discuss the various histological differential diagnosis and prognostic factors along with a brief review of the literature. A 41-year-old male patient presented with gradually enlarging mass per abdomen of 2 months duration associated with pain since one week. Local examination revealed a hard palpable mass extending from epigastric to umbilical region. Borders were not well defined. His post prandial blood sugar was 54 mg/dl and ESR was 55 mm/hr. All other laboratory parameters were within normal limits. Computed tomography (CT) examination revealed a large well defined heterogenously enhancing abdomino-pelvic mass lesion in the midline extending from L1-S2 vertebral levels, displacing the bowel loops and vessels to the periphery [Figure - 1]. Exploratory laparotomy with excision of the mesenteric tumor was done and the specimen received for histopathological examination. Pathological findings Grossly, the tumor consisted of a well circumscribed round to oval mass weighing 1057 gm and measuring 23 × 20 × 9 cm. Cut section showed variegated appearance with grey white, yellow, hemorrhagic, and focal cystic areas [Figure - 2]. Histopathology sections showed plump spindle cells with round to oval nucleus, granular chromatin, inconspicuous nucleoli, and scant eosinophilic cytoplasm arranged in "patternless pattern" with interspersed fibrous bands and ropy collagen. Ectatic blood vessels, broad zones of hyalinization, areas of necrosis, and foci of increased cellularity were noted with a mitotic count of 2-4/10 hpf. Cellular pleomorphism was inconspicuous. The tumor cells were strongly positive for cluster of differentiation 34 (CD34) and CD99. A few dispersed cells were S-100 positive [Figure - 3], [Figure - 4], [Figure - 5] and [Figure - 6]. C-kit and EMA (epithelial membrane antigen) were negative. Based on histopathology, immunohistochemistry, and large tumor size (>10 cm), a final diagnosis of benign GSFT of the mesentery was made. Seven months follow-up of the patient showed no evidence of tumor recurrence. His blood sugar levels were normal at the time of last follow-up. SFTs were first described by Klemperer and Rabin in 1931 as pleural based tumors of submesothelial origin. Currently, there is a consensus that SFT is a distinctive mesenchymal neoplasm which ultrastructurally displays features of pericytic, fibroblastic, and/or myofibroblastic differentiation. [1] Extrapleural SFTs are uncommon tumors of ubiquitous location which are quite similar clinically and biologically to their pleural counterparts. Specific symptoms relate to the location of the tumor. They are generally benign, slow-growing neoplasms with favorable prognosis; however, malignant variants have also been reported. The average size of these tumors ranges from 5-8 cm. [2] Tumors larger than 10 cm in size are called ′giant SFTs′. Review of the literature revealed only 8 cases of GSFTs in extra-pleural sites. The clinical details, treatment given and outcomes of these cases along with the present case have been enlisted [Table - 1]. Around 5% of the tumors secrete insulin-like growth factors (IGFs) contributing to the associated hypoglycemia (so called Doege-Potter syndrome). [1],[3] This was also observed in our case. SFTs are broadly categorized under HPC-like tumors. [1 Microscopic examination shows spindle cells dispersed among elongated dense collagen fibers in a "patternless" pattern and around thin walled blood vessels. The nuclei are usually bland and mitoses are rare (1-2 mitosis/10 hpf). [5] Majority of the tumors pursue a favorable clinical course. Although tumor size has been reported as a prognostic factor, review of the literature reveals that large tumor size is not necessarily a marker of malignancy. Malignancy in SFT should be suspected if at least 3 of these 4 criteria are present: mitosis (>4/10 hpf), high cellularity, necrosis, and presence of nuclear atypia. [11] The current case showed <4 mitosis/10 hpf, focal hypercellularity, and necrosis with no nuclear atypia. Moreover, the tumor was well circumscribed with no infiltrative margins. Benign tumors are treated with en-block surgical resection. Kumavara et al., [6] observed that malignant tumors needed tfurther treatment with RT proving more useful than ChT. Recurrence has been observed to be higher in tumors with malignant histology, sessile morphology, cytokeratin positivity, and decreased expression of progesterone receptor. Intra abdominal tumors included in the histological differential diagnoses of SFTs include: gastrointestinal stromal tumor (GIST), malignant peripheral nerve sheath tumor (MPNST), and synovial sarcoma (SS). All these tumors are composed of spindle cells with HPC-like areas. Immunohistochemistry has a central role in differentiating them. In the present case, C-kit negativity helped us to exclude GIST. MPNST shows more diffuse positivity with S-100 and is negative for CD34 and CD99. The present case showed occasional S-100 positive cells. However, 5 to 10% of SFTs′ have been observed to show scattered S-100 positive cells. [12] SS was ruled out as EMA was negative. To conclude, SFTs are uncommon, slow growing tumors and can reach large sizes (10 cm to > 30 cm) when they are called GSFTs. In spite of their large size, most giant SFTs described in the literature did not show evidence of recurrence, thus highlighting the fact that GSFTs can be benign. CD34 immunohistochemistry is crucial for diagnosing SFT and to exclude other histological mimics. Unlike other spindle cell tumors which may require additional chemo/radiotherapy, an en-block surgical excision is adequate treatment for benign SFTs. Acknowledgement We wish to extend our appreciation to Mr Ganesh Prasad, Artist, Department of Pathology- KMC Manipal, for the help rendered in compiling the photographs. References
Copyright 2011 - Journal of Cancer Research and Therapeutics The following images related to this document are available:Photo images[cr11096t1.jpg] [cr11096f6.jpg] [cr11096f2.jpg] [cr11096f4.jpg] [cr11096f3.jpg] [cr11096f1.jpg] [cr11096f5.jpg] |
| |||||||||


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}