 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
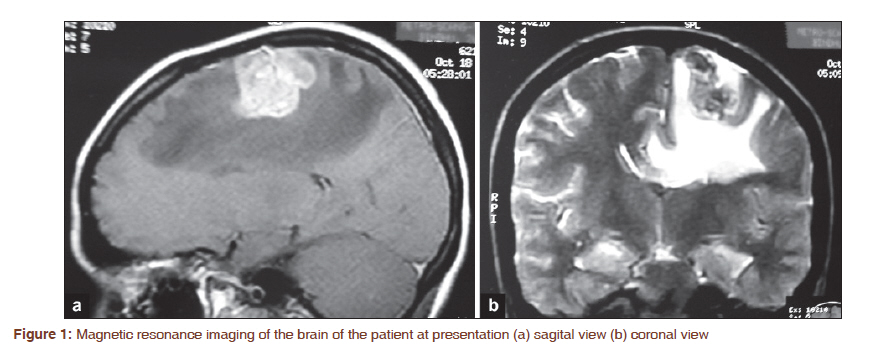
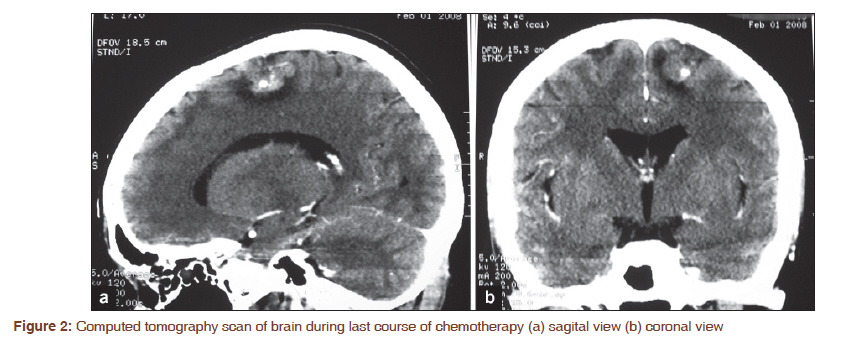
Journal of Cancer Research and Therapeutics, Vol. 7, No. 3, July-September, 2011, pp. 383-384 Letter to the Editor - Documenting a Case Choriocarcinoma with brain involvement Francis V James1, Attokaran L Lijeesh1, Sumod M Koshy2, Aswin Kumar1 1 Division of Clinical Oncology, Regional Cancer Centre, Trivandrum, Kerala, India Sir, It was interesting to read the case report by Ravi Dadlani and team in JCRT on choriocarcinoma metastatic to brain. [1] There are few observations and comments. First point, it is mentioned that "to obtain a conclusive diagnosis," a second decompressive surgery was done for medial frontal lesion. Already this young lady had an evacuation of right parietal hematoma and had computed tomography scan evidence of liver, spleen, and pelvic disease, and an estimation of beta human chorionic gonadotrophin (HCG) would have made the diagnosis. In the case of metastatic brain disease from choriocarcinoma, early institution of chemotherapy is an important factor as the disease advances rapidly and raised beta HCG would be adequate to start treatment and histological confirmation is not mandatory. Intracranial hemorrhage as a feature of choriocarcinoma was reported in a series of 10 cases from India previously. [2] Second smaller point is on commencing "adjuvant" chemotherapy. This term is inappropriate and it has to be clearly understood that chemotherapy is the primary treatment for choriocarcinoma and is curative and not adjuvant. Third point is regarding EMACO schedule which is a biweekly course and is described with long gaps in [Table 1]. We also wish to share a report from our center, where a 26-year-old lady presented with right-sided hemi paresis of grade 3 and history of seizures on 22.10.2007. Her magnetic resonance imaging showed space occupying lesion with hemorrhage and perilesional edema of left parietal region [Figure - 1]a and b. She had previous normal delivery 18 months ago. Her beta HCG was increased at 52116 m U/ml. There was no evidence of disease in chest or abdomen on imaging. She was treated with whole brain radiotherapy 30 Gy in 15 fractions over 3 weeks and EMACO chemotherapy. Her Beta HCG normalized after three cycles and continued for three more cycles until 06.02.2008. The computed tomography scans during sixth course are shown in [Figure - 2]a and b, which did not show any evidence of disease except calcification. She has delivered a normal girl in January 2010. In February 2010, she had focal seizure, and repeat magnetic resonance imaging revealed no signs of recurrence and was advised to continue anti-epileptics. When last reviewed in April 2011, she remained well 38 months after treatment. Management of Gestational Trophoblastic Disease with brain involvement is challenging, yet cure rate is high. [3] Treatment is primarily by chemotherapy with surgery and or radiotherapy in selected cases. References
Copyright 2011 - Journal of Cancer Research and Therapeutics The following images related to this document are available:Photo images[cr11099f1.jpg] [cr11099f2.jpg] |
| |||||||||


{kind=link}
{kind=link}