 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
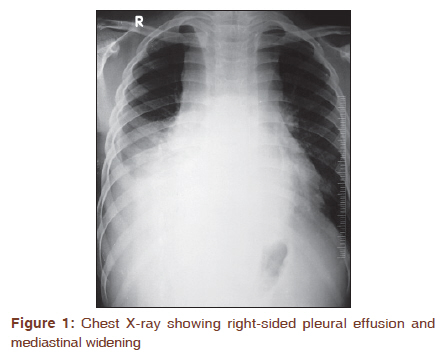
Journal of Cancer Research and Therapeutics, Vol. 7, No. 3, July-September, 2011, pp. 389-390 Letter to the Editor - Documenting a Case Hand-mirror cell morphology of T-cell lymphoproliferative disorder presenting in pleural effusion with mediastinal widening Mani Anand, Harveen K Gulati, Avinash R Joshi Department of Pathology, Smt. Kashibai Navale Medical College and General Hospital, Narhe, Pune, Maharashtra, India PMID: 22044839 DOI: 10.4103/0973-1482.87032 A 13-year-old boy came with complains of cough, breathlessness, and chest pain of 8 days duration which rapidly progressed to severe respiratory distress in the past 24 h. His past medical history was unremarkable. Physical examination revealed bilateral cervical lymphadenopathy. Peripheral blood showed a hemoglobin of 9.9 g/dl, total leukocyte count of 15.9 × 10 9 /l with normal differential, and a platelet count of 111 × 10 9 /l. Rest of the routine haematological and biochemical investigations were within normal limits. Chest X-ray revealed right-sided pleural effusion with mediastinal widening [Figure - 1]. Pleural fluid was tapped to relieve the respiratory distress. Cytological examination of pleural fluid sample showed a monomorphic population of cells with "hand-mirror" cell morphology. These cells exhibited cytoplasmic extensions (uropodia) with three to five coarse dark cytoplasmic granules and a rim of vacuolated cytoplasm capping the opposing "mirror head" side. Occasional mitoses and apoptotic cells were also noted. The background showed few mesothelial cells and macrophages [Figure - 2]. These atypical lymphoid cells on immunocytochemistry showed positivity for CD3 and were non-reactive for CD20. Following this, a bone marrow examination was performed which was within normal limits. These findings collectively supported the diagnosis of a T-cell lymphoproliferative disorder with predominant hand-mirror cell morphology. The patient succumbed to the disease within 2 days of hospital admission which did not allow for further histological evaluation of the mediastinal mass or the enlarged cervical lymph nodes. Malignant effusions can be broadly considered to fall into three main groups: (1) obvious population of abnormal cells, dissimilar to mesothelial cells; (2) abnormal cells similar to mesothelial cells; and (3) abnormal lymphoid cells within a background of usual mesothelial cells and macrophages. Effusions caused by lymphomas usually involve other body sites before the body cavities. [1] On the other hand, primary body cavity lymphoma (primary effusion lymphoma) generally presents as a large B-cell lymphoma involving the pleural, pericardial, or peritoneal cavities first. These cases have been associated with HIV infection, immunocompromised transplant recipients, or with either Herpesvirus-8 and Epstein-Barr virus. [2] Cells with "hand-mirror" morphology have rarely been described in a primary effusion fluids. The cell is characterized by an asymmetrical cytoplasmic elongation extending out from one pole of the nucleus (uropod). Both the nucleus and the elongated cytoplasmic "handle" together give the appearance of a hand- mirror. Hand-mirror cells should be differentiated from reactive mesothelial cells which at times may mimic these cells. Single mesothelial cell seen in body fluids are spherical or oval and measure between 15- and 20 μm in diameter. The cyanophilic or faintly eosinophilic cytoplasm is sharply demarcated and shows two cytoplasmin zones: a perinuclear denser zone and a peripheral clear zone. Their nucleus is round to oval, generally located at the centre of the cell, of even size, sharply demarcated, slightly granular, and contains one or two, centrally located, readily visible nucleoli. A characteristic feature of mesothelial cells in doublets or small linear clusters is the flattening of the opposite cell membranes with formation of a clear gap or "window". These "windows" are due to microvilli separating the cells. On electron microscopy, the mesothelial cells are characterized by the presence of regular short microvilli or a mixture of microvilli with bleb-like structures. [3] On the other hand, hand-mirror cells on ultrastructural examination exhibit long cytoplasmic projections, accounting for the "handle" of these cells. [4] Immunohistochemical evaluation of hand-mirror cells requires a panel of lymphoid markers including leukocyte common antigen, a pan B-cell marker such as CD20, and a pan T-cell marker such as CD3. [5] All the above markers will be negative in reactive mesothelial cells. Hand-mirror cells have been reported with many diagnostic entities including cutaneous natural killer cell lymphomas, anaplastic Ki-1 lymphoma, acute lymphoblastic leukemia, Burkitt′s lymphoma, other B-cell lymphomas with surface IgM-lambda, and with granulocytic and acute myelomonocytic leukemia. [1] The distinct morphology most likely represents an aspect of immune responsivity or challenge involving the incorporation of immune complexes. [4] Although an easily recognized morphologic form, the hand-mirror cell morphology has generally been considered to be of limited prognostic value with the exception that the recognition of this morphology points to a lymphoid lineage. [6] Chemotherapy forms the main line of management in these cases. The prognosis is poor with a high relapse rate. [7] References
Copyright 2011 - Journal of Cancer Research and Therapeutics The following images related to this document are available:Photo images[cr11103f1.jpg] [cr11103f2.jpg] |
| |||||||||


{kind=link}
{kind=link}