 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
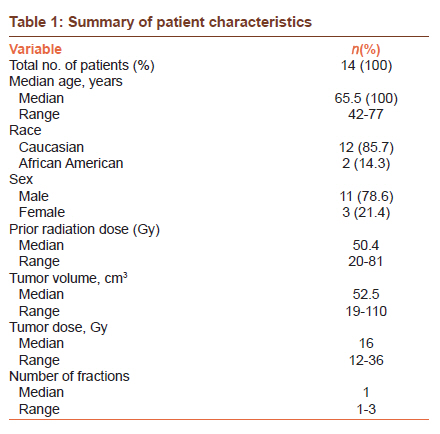
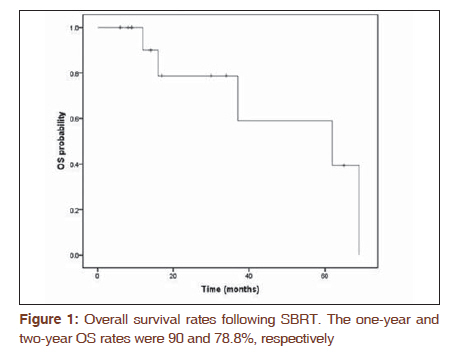
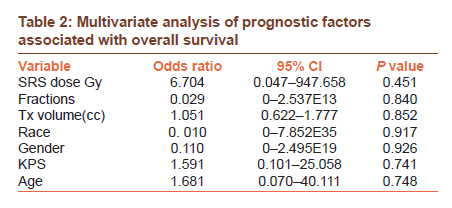
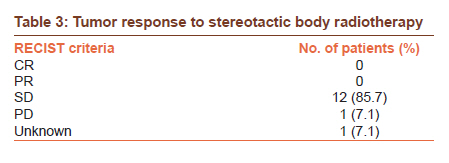
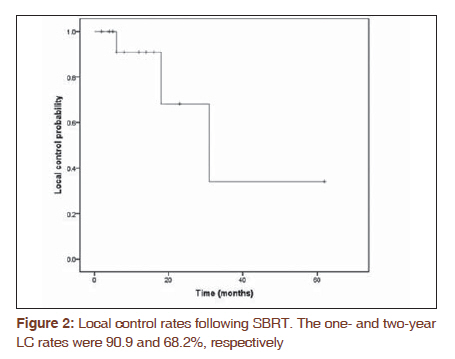
Journal of Cancer Research and Therapeutics, Vol. 7, No. 4, October-December, 2011, pp. 408-411 Original Article Stereotactic body radiotherapy for the treatment of presacral recurrences from rectal cancers Sarahgene G DeFoe1, Mark E Bernard1, Jean-Claude Rwigema1, Dwight E Heron2, Cihat Ozhasoglu1, Steven Burton1 1 Department of Radiation Oncology, Head and Neck Surgery, University of Pittsburgh Cancer Institute, Pittsburgh, PA 15232, USA Code Number: cr11111 DOI: 10.4103/0973-1482.92000 Abstract Purpose: Management of recurrent presacral rectal cancer is often not amenable to curative surgery. The goal of this study is to evaluate the safety and efficacy of cyberknife stereotactic body radiotherapy (SBRT) in the management of presacral recurrences. Keywords: Cyberknife, pain, reirradiation Introduction Management of patients with rectal cancer is often times intensive and usually requires pre-operative chemoradiation therapy as an integral part of therapy. Recurrent disease in the pelvis carries a poor prognosis with a medium survival ranging from 3.5 to 10.5 months without treatment. [1],[2],[3] Patients with metastatic tumors involving the pelvis are often not candidates for curative resection as frequently oligometastatic disease is often present and the surgical risk may outweigh its benefit. [1] However, without local therapy, patients with pelvic tumors are likely to experience progressive, severe symptoms, especially pain, which can significantly impact the quality of life. [4],[5] There is no standard for the treatment of locally-recurrent rectal cancer in the presacral area. [1] Chemotherapy or external beam radiation therapy may only provide temporary relief. Most of these patients have already received maximum dose to normal tissues in the pelvis such as the bowel and bladder making re-treatment with conventional radiation therapy impossible due to the high risk of radiation-induced complications. Stereotactic body radiotherapy (SBRT) is an emerging technology in the radiation oncology field. This technique utilizes stereotactic principles for localization and delivers multiple beams of radiation to well-defined targets in few fractions. Therefore, SBRT can deliver higher doses to the tumor and while limiting normal tissue toxicity. The goal of this study is to evaluate the safety and efficacy of SBRT in the treatment of metastatic pelvic tumors as well as to evaluate long-term survival and local control and toxicities of treatment. Materials and Methods Patients with recurrent, unresectable or previously-irradiated malignancies in the presacral region of the pelvis who were treated with SBRT using the Cyberknife Radiosurgical System (Accuray Inc., Sunnyvale, CA, USA) were the subjects of this study. All patients were treated at the University of Pittsburgh Cancer Institute and signed a written informed consent. The institutional review board approved the protocol and data was retrospectively acquired and de-identified according to the Health Insurance Portability and Accountability Act guidelines. Presacral tumors were defined as tumors located in the anterior portion of the sacrum below the second segment (S2-S5). At least three gold fiducial markers were placed percutaneously in or near the tumor by the referring surgeon or by interventional radiology. All patients underwent CT simulation in the treatment position (supine) with a customized body immobilization system. The images were sent to the radiosurgical planning system and target volume was contoured on axial CT images. The target volume was defined as the gross tumor volume (GTV). The GTV was considered identical to the clinical target volume (CTV). A 5-mm margin was added to the GTV to create the planning target volume (PTV) to account for set-up uncertainty. The radiation dose was delivered either as a single-dose or fractionated regimen (<5 treatments). Radiation doses were prescribed to the 80% isodose line of the maximum dose to cover the 98-99% of the PTV. The fractionated SBRT was given with 36 Gy in 3 fractions 2-3 times per week. The single SBRT dose was given with single doses of 12, 16 or 18 Gy. The choice of fractionation was based mostly on tumor volume, and location of the tumor and prior radiation dose. Other factors, such as prior radiation treatment, adjacent normal tissue, and the patient's general condition and comorbidities were also taken into consideration in treatment selection. All patients were evaluated by a multi-disciplinary team consisting of radiation, medical and surgical oncology one month after the completion of treatment and then every three to six months for an year then yearly thereafter. At each follow-up, patients underwent a complete physical examination. Imaging studies were performed at the discretion of the treating or referring physician or as indicated by clinical findings. Tumor response to treatment was assessed using modified response evaluation and criteria in solid tumor (RECIST) which specifies tumor response as either complete response (CR), partial response (PR), stable disease (SD), or progressive disease (PD). [6] Local failure was defined as a 20% increase in the sum of the longest diameter of target lesion in keeping with the RECIST criteria. If a new lesion developed in the pelvis but outside the radiation field, it was interpreted as distant metastasis. Acute and late toxicities were defined as symptoms that developed within three months post-SBRT or later, respectively. The Common Terminology Criteria for Adverse Events (CTCAE) version 3.0 was used for toxicity scoring. Survival endpoints were calculated from the date of treatment completion and estimated using the method described by Kaplan and Meier. [1] Local recurrence-free survival (LRFS) was defined as time to local treatment failure. Statistical analyses were performed using SPSS version 17.0 (SPSS Inc., Chicago, IL). Cox regression was used to model predictors of outcome. Results Patient characteristics Between April 2003 and October 2008, 14 patients with presacral tumors from rectal cancer were treated with SBRT using the Cyberknife system at the University of Pittsburgh Medical Center. The median age of the study population was 65.5 years (range, 42-77 years), and there were 11(78.6%) men and 3(21.4%) women. One patient (6.7%) received SBRT as part of a boost. Prior median dose to the pelvis was 50.4 Gy (range, 20-81 Gy). Median tumor volume was 52.5 cm3 (range, 19 - 110 cm3 ) in the pelvic area involving either soft tissues (n=8), bone (n=1) or both (n=2). Median tumor dose was 16Gy (range, 12-36 Gy) with a median fractionation of 1 (range, 1-3 Gy). All patients underwent previous treatment for rectal cancer. Patient, tumor and treatment characteristics are outlined in [Table - 1]. Survival Median follow-up time was 16.5 months (range, 6-69) and no patient was lost to follow-up. The one-year and two-year OS rates were 90 and 78.8%, respectively [Figure - 1]. On multivariate analysis, SBRT dose, number of fractions, tumor volume, race, gender, and KPS were not predictors of overall survival [Table - 2]. Local control At initial follow-up of a median 4.9 months (1 - 16.3 months), treatment responses were complete response (n=3) and stable disease (n=8). Median time to evaluating treatment response was four months, range (1-24). [Table - 3] lists the response based on RECIST criteria. Out of the 14 patients, 12(85.7%) had stable disease and 1 (7.1%) developed progressive disease. The one- and two-year LC rates were 90.9 and 68.2%, respectively [Figure - 2]. On multivariate analysis, SBRT dose, fractions, tumor volume, race, gender, or KPS were not found to be predictors of local control. Pain relief Initially, 7 (50%) reported pain symptoms due to tumor prior to SBRT; of those, 4 (57.1%) patients reported no need of pain medications post-treatment. Toxicity There were no reported grade 3 or 4 genitourinary, gastrointestinal, or neurologic toxicities in this cohort of patients. One patient developed a recurrent pelvic abscess after SBRT, which required evacuation and drainage. Discussion The management of patients with locally-recurrent rectal cancer in the presacral area remains challenging. Clinicians are compelled to make the best therapeutic decisions of imperfect options for these patients with limited data to support therapeutic interventions. Prior to the advent of total mesorectal surgery (TME), the local recurrence rate following curative surgery ranged from 12% to 38%. [5],[7],[8] With the advent of TME combined with adjuvant therapy, many series have reported local recurrence values to be 13% or below. [5],[9],[10] Despite aggressive multimodality management, local control remains as a challenge necessitating local radiation therapy to minimize the risk of recurrence. Most of these patients are not candidates for curative resection and the median survival for locally-recurrent rectal cancer is eight months with patients experiencing pain and poor quality of life. [1] While several studies have evaluated the therapeutic outcomes to various treatment strategies (e.g. radiation, surgery, and chemotherapy) for management of localized pre-sacral recurrences, radical surgery is seldom a viable option since recurrence is predominately detected as a fixed mass invading the sacrum and or pelvic wall. [1] These cases of local recurrence require extensive surgery such as pelvic exenteration or abdomino-sacral resection to attain satisfactory margins. However, these surgical requirements are associated with very high perioperative morbidity rates ranging from 42% to 59%, which reduces quality of life. [4],[5] Therefore, a radiotherapeutic option to both aggressively treat the tumor with minimal toxicities would be desirous. Results from this study have demonstrated the feasibility of SBRT as a viable treatment modality for locally-recurrent rectal cancer in the presacral area. SBRT is an ideal modality as a result of its capabilities to deliver a highly focused dose of radiation while limiting injury and normal tissue toxicities. There is limited data describing the effectiveness of SBRT as a single treatment modality for locally recurrent rectal cancer in the presacral area. Kim et al reported a four-year local control rate of 74.3% with 1 patient having grade 4 toxicities. [1] This patient had received 51Gy, a much higher dose than what we prescribed. We report a local control rate of 90.9% at one-year with no reported grade 3 or 4 genitourinary, gastrointestinal, or neurologic toxicities. Kim et al also reported 9 (39%) of their 23 patients having grade 1 or 2 toxicities either during treatment or for a diminutive period of time after treatment while we did not report any. The higher LC rate and higher amount of toxicities shown by Kim is most likely secondary to the higher dose range used (i.e. 30-51Gy). Several studies have evaluated the therapeutic outcomes of combination therapy as well as surgery as a standalone treatment for patients with recurrent rectal cancer.[2],[11],[12],[13],[14] The five-year overall survival after complete resection has ranged from 19% to 55% with the higher survival attributable to the selection of patients with a resectable mass at the time of recurrence.[1] Despite the probability of selection bias in the literature, our one-year and two-year overall survival using SBRT for recurrent rectal cancers in the presacral area are comparable to what is reported from multiple modality studies. Bussières et al used a multimodality approach with intraoperative radiotherapy (IORT) for the treatment of recurrent rectal carcinomas and showed one- and two-year OS rates of 72.40 and 44.60%.[11] Both of these values are lower than what we reported (i.e. 90 and 78.8%). Most of our patients (57.1%) who experienced pain prior to SBRT did not require pain medications following treatment suggesting the possible palliative efficacy of SBRT in this setting. SBRT appears to provide acceptable local control and limited normal tissue toxicity while improving pain as a minimally-invasive procedure. This is an attractive feature in this patient population. Conclusions SBRT is a safe and efficacious treatment option for patients with presacral failures from primary rectal carcinomas. Comparable OS rates compared to a multimodality approach were achieved. Acknowledgements We would like to acknowledge Annette Quinn, R.N., M.S.N for her dedicated work with our service. References
Copyright 2011 - Journal of Cancer Research and Therapeutics The following images related to this document are available:Photo images[cr11111f2.jpg] [cr11111f1.jpg] [cr11111t3.jpg] [cr11111t2.jpg] [cr11111t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}