 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
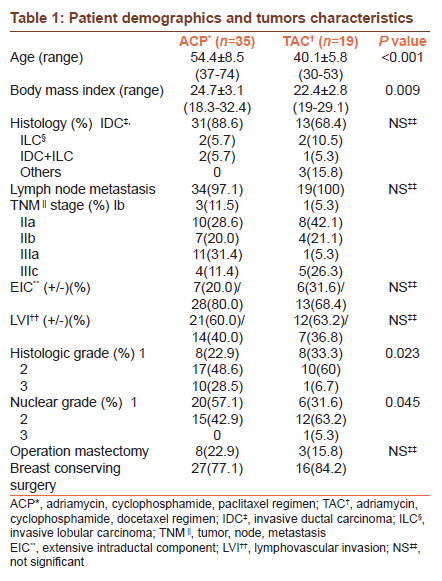
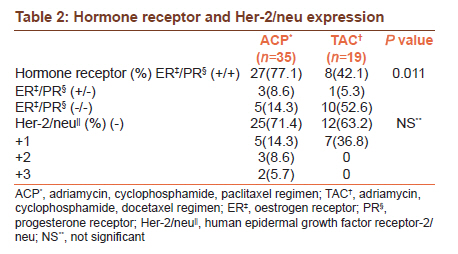
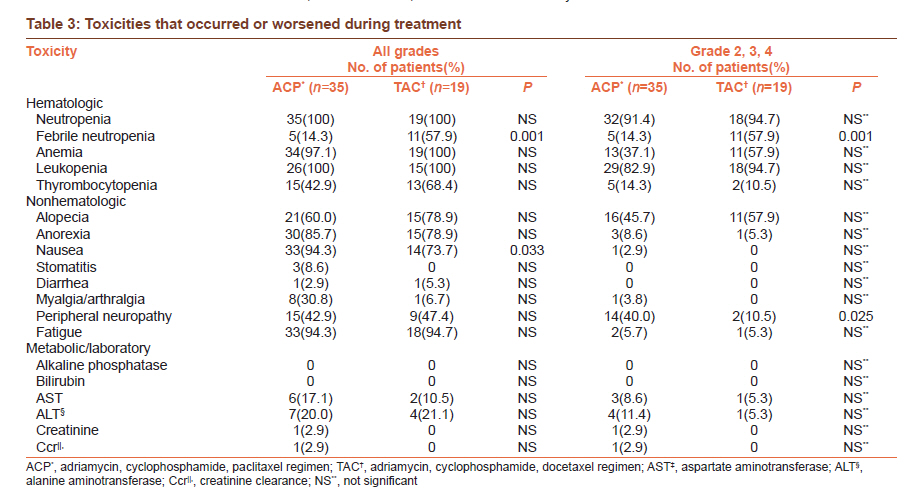
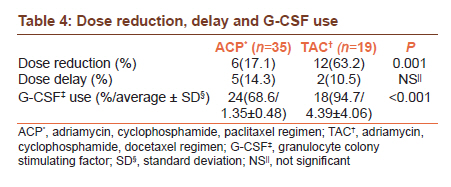
Journal of Cancer Research and Therapeutics, Vol. 7, No. 4, October-December, 2011, pp. 412-415 Original Article Toxicities, dose reduction and delay of docetaxel and paclitaxel chemotherapy in breast cancer without distant metastases Woo Young Kim1, Sang Uk Woo1, Jae Hong Seo2, Gil Soo Son3, Jae Bok Lee1, Jeoung Won Bae4 1 Department of Surgery, Guro Hospital, Korea University College of Medicine, Seoul, Korea Code Number: cr11112 DOI: 10.4103/0973-1482.92004 Abstract Background: Docetaxel and paclitaxel are likely to have different toxicity profiles, dose reduction and delays despite their similar medical results in breast cancer patients. Keywords: Dose delay, dose reduction, docetaxel, febrile neutropenia, paclitaxel, peripheral neuropathy, toxicity Introduction Taxanes are some of the most active agents against breast cancer. Positive outcomes with taxanes in breast cancer chemotherapy have been reported in an adjuvant setting. Until the 1990s, anthracyclines were considered to be the most active agents and were used in both adjuvant and metastatic settings. Both anthracyclines-taxanes combinations were shown to improve response rates and progression-free survival (PFS) significantly compared to treatment without taxane. [1],[2],[3] Both anthracyclines-taxanes combinations yield similar results in terms of the overall survival(OS) and progression-free survival (PFS) in metastatic breast cancer. [4],[5] Nevertheless, they are likely to have different toxicity profiles, such as peripheral neuropathy, neutropenia, neutropenic fever, etc. The current evaluation was carried out to evaluate retrospectively the incidence and severity of certain toxicities and dose reduction, delay, G-CSF use of two taxanes (docetaxel, paclitaxel) in clinical practice at a single institution multidisciplinary breast center. Materials and Methods From January 2009 to June 2010 in a single institution multidisciplinary breast center, this study enrolled 54 patients with lymph node-positive (tumor stage T1, T2, or T3 and nodal stage N1 or N2) and high risk, node-negative (T2 or T3, N0) breast cancer without distant metastases, who received adjuvant chemotherapy. Thirty five patients received adrimycin, cyclophosphamide (60/600 mg/m 2 ) for four cycles followed by paclitaxel (Genexol® ; Samyang, Seoul, Korea) (175 mg/m 2 ) and 19 received adrimycin, cyclophosphamide, docetaxel (Taxotere® ; Aventis Pharma S.A, France) (60/600/100mg/m 2 ) for six cycles in every three weeks. The decision to administer paclitaxel or docetaxel was based on the drug availability, age, body mass index (BMI), etc. Before each cycle, toxicity assessment, physical examination, complete blood counts and biochemical profile, dose reduction, delay in previous cycles and G-CSF use were evaluated. A dose reduction by one dose level was performed in any case with the following dose-limiting toxicities: absolute neutrophil count (ANC) < 0.5 × 10 9 /L for >7 days, ANC < 0.1 × 10 9 /L for >3 days, grade 3 or 4 thrombocytopenia for >7 days, increase of transaminase by ≥50%, severe (grade 3 or 4) mucositis, neuropathy, myalgia or arthralgia not responding to symptomatic treatment. A dose delay was performed in cases with infectious diseases, delayed recovery from infection or febrile neutropenia. The toxic effects were graded according to the National Cancer Institute Common Toxicity Criteria, version 3.0 Characteristics. Informed consent was obtained for all patients. Toxicities, dose reduction and delay, G-CSF use between the two groups were compared using Mann-Whitney test and Fisher's exact test. A P value < 0.05 was considered as significant. Results [Table - 1] and [Table - 2] list the details of the patients' demographics, tumor characteristics and hormone receptor, Her-2/neu expression, respectively. A total of 114 cycles and 280 cycles were administered to the patients in the TAC and ACP group, respectively. No patient refused to continue chemotherapy due to intolerance to the chemotherapy. Overall, the mean age and BMI was 48.6 (range from 30 to 74) and 23.9 (range from 18.3 to 32.4), respectively. Increasing age was associated with an increased risk of anemia (P=0.004), fatigue (P=0.009) and pain (P=0.003), and a decreasing BMI was associated with an increased risk of febrile neutropenia (P=0.009) (data not shown). The mean age of the patients in the TAC and ACP group were 40.1±5.8 (range from 30 to 53) and 54.4±8.5 (range from 37 to 74), respectively (P<0.001). The mean BMI of the two groups were 22.4±2.8 and 24.7±3.1, respectively (P=0.009). The histologic grade (P=0.023), nuclear grade (P=0.045) and hormonal receptor (ER/PR) (P=0.011) of the two groups were significantly different. [Table - 3] lists the incidence and severity of toxicity by treatment protocol. For non-hematologic toxicity, patients in the TAC group experienced alopecia more frequently than those in the ACP group. Patients in the ACP group experienced peripheral neuropathy (P=0.025) (excluding grade 0/1), nausea (P=0.033) (all grades) more frequently than those in TAC. One patient in the ACP group had transient, reversible renal function impairment. In the hematologic toxicity, grade 2/3/4 neutropenia was more common in the TAC group (n=18, 94.7%) but this was not significant. Febrile neutropenia occurred in 11 (57.9%) and five (14.3%) patients in the TAC and ACP group, respectively (P=0.001). G-CSF use was performed on 24(68.6%) and 18(94.7%) patients in the ACP and TAC group, respectively (P<0.001) [Table - 4]. On the other hand, anemia was not significantly more common in the TAC group. Two and four patients in the TAC and ACP group, respectively, experienced grade 2/3/4 thrombocytopenia. Dose reduction (one level dose) was performed in 6(17.1%) and 12(63.2%) patients in the ACP and TAC group, respectively (P=0.001)[Table - 4]. Dose delay was performed in five (14.3%) and two (10.5%) patients in the ACP and TAC group, respectively. Among them, four patients had a dose delay due to an increase in the transaminase level and each of the others had dose delay due to influenza, delayed recovery from febrile neutropenia and knee cellulitis respectively. A dose reduction only was significant (P= 0.001). Discussion The decision to offer chemotherapy to patients with breast cancer is difficult and chemotherapy- related toxicity must be considered carefully. The ECOG 1199 trial evaluated both taxanes (docetaxel and paclitaxel) and examined the optimal administration route for improved clinical efficacy. [5] After a median follow-up of 63.8 months, there were no significant differences in the hazard ratios of the disease-free survival when comparing the two taxanes (hazard ratio [HR] = 1.02, P = 0.73) or two schedules (weekly versus in every three weeks)(HR = 1.07, P = 0.3). [5] Although taxanes in clinical practice prolong remission and improve survival, they are also associated with a significant occurrence of toxicity. [6] In several trials including ECOG 1199, in addition to neutropenia, other toxicities that occurred more frequently in docetaxel than paclitaxel included thrombocytopenia, anemia, need for blood transfusions, mucositis, nail disorders, skin toxicity, chemotherapy-related amenorrhea, asthenia, edema and infection. [2],[5],[7],[8] In trials of taxanes-containing regimens, the most common serious toxicity was myelosuppression. Grade 4 neutropenia develops in 85-100% of patients and febrile neutropenia occurs in 30-40% of patients at some time during treatment. [9],[10] According to the guidelines developed by organizations, such as the American Society of Clinical Oncology, [11] the incidence of febrile neutropenia suggests that the use of hematopoietic growth factors should be considered. The present study also used prophylactic G-CSF in both regimens if grade 4 neutropenia or febrile neutropenia were encountered. Docetaxel was associated with less nausea and vomiting. Paclitaxel was associated with more peripheral neuropathy and hypersensitivity reactions. [8] The primary target of taxanes-induced peripheral neuropathy (TIPN) is controversial. Studies in preclinical models demonstrated that the administration of paclitaxel resulted in the accumulation of microtubules in Schwann cells and axons of the sciatic nerve. The main occurrence of distal loss of sensation in the large fibers would suggest that a "dying back" process starting from the distal nerve endings followed by effects on Schwann cells, neuronal body or disturbed axonal transport changes in the affected neurons is the mechanism of TIPN. [12] The incidence and severity of TIPN in paclitaxel is higher than that in docetaxel. [13] For the symptomatic management of TIPN, amitriptyline, glutamine, low-dose oral prednisone and gabapentin have been used with some measure of success for reducing pain, myalgia and arthralgia. [12] Neutropenic events are associated with higher age, higher body surface area, lower body mass index, regimen type, and more planned chemotherapy cycles. [14] Overweight patients are less likely to experience cycle delays due to prolonged myelosuppression, particularly toward the end of the treatment course. Overall, obese patients are in fact less likely to suffer hematologic toxicity. Healthy older patients without comorbidity had a higher rate of hematologic toxicity than younger patients, but no increase in nonhematologic toxicity. [15],[16] Elderly patients treated with newer adjuvant chemotherapy regimens derive the same benefits from newer chemotherapy regimens as younger patients but should be cautioned about the increased risk of toxicity and treatment-related death. [16] Consistent with the two trials, in the present study, increasing age was associated with an increased risk of anemia (P=0.004), fatigue (P=0.009) and pain (P=0.003), and a decreasing BMI was associated with an increased risk of febrile neutropenia (P=0.009) (data not shown). In one meta-analysis, significant dose reductions and delays are common clinical practice in the management of patients with primary breast cancer. An even more alarming picture might be observed in patients with metastatic breast cancer, where dose delays and reductions are common methods of reducing the toxicity and maintaining the quality of life. [17] Dose reduction and delay have no negative influence in the short run but the overall survival was better in patients with fewer dose reductions and delays. On the other hand, this study did not evaluate the impact of dose reduction and delay on the short and long-term outcome due to the short follow-up. In conclusion, there were two significant differences in toxicity, febrile neutropenia and peripheral neuropathy, between the two taxanes. Dose reduction and G-CSF use were performed more frequently in the TAC group than the ACP group. A taxane-based regimen should be chosen for patients with advanced breast cancer based on the pharmacokinetics, dosing schedule, clinical activity and toxicity profile that best meet the patient's therapeutic needs and quality of life. Moreover, a dose reduction and delay should only be undertaken for important reasons, such as unacceptable toxicity impairing the quality of life. References
Copyright 2011 - Journal of Cancer Research and Therapeutics The following images related to this document are available:Photo images[cr11112t4.jpg] [cr11112t1.jpg] [cr11112t2.jpg] [cr11112t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}