 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
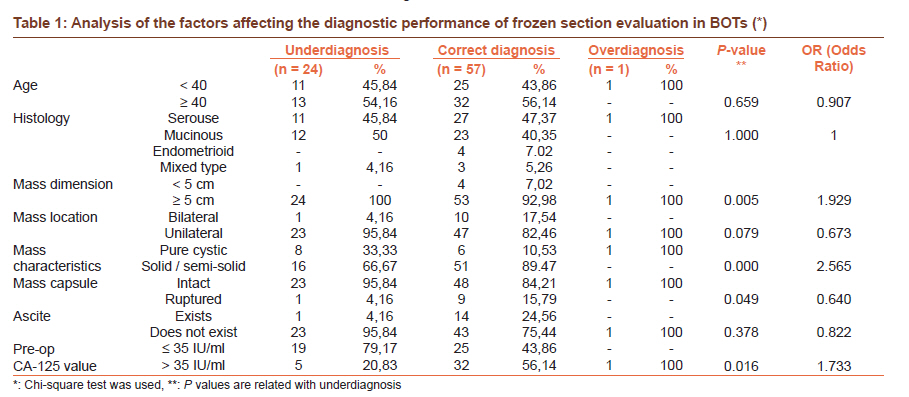
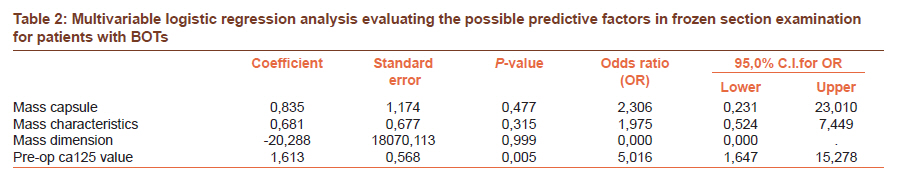
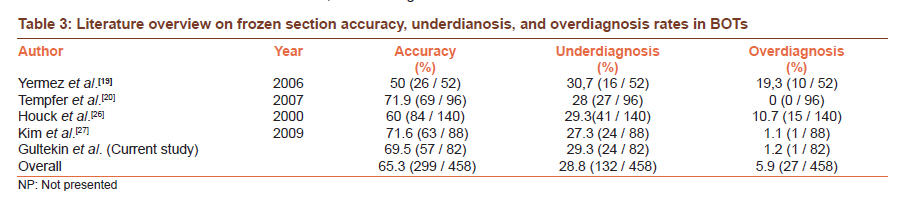
Journal of Cancer Research and Therapeutics, Vol. 7, No. 4, October-December, 2011, pp. 416-420 Original Article The value of frozen section evaluation in the management of borderline ovarian tumors Emre Gultekin1, Ozge Elmastas Gultekin2, Basak Cingillioglu1, Sevil Sayhan3, Muzaffer Sanci1, Yusuf Yildirim1 1 Department of Gynecologic Oncology, Ege Gynecology and Maternity Training and Research Hospital, Yenisehir, Izmir, Turkey Code Number: cr11113 DOI: 10.4103/0973-1482.92005 Abstract Purpose: To evaluate the accuracy of a frozen section and to analyze the factors affecting frozen section results in cases of borderline ovarian tumors (BOTs). Keywords: Borderline ovarian tumors, frozen section, overdiagnosis, underdiagnosis Introduction Borderline ovarian tumors (BOTs) are a heterogenous group of lesions, which differ from invasive epithelial ovarian tumors through the lack of stromal invasion, in spite of having epithelial proliferation and atypia. [1] Borderline ovarian tumors consist of 10 - 20% of all ovarian malignancies. [2] In contrast to invasive epithelial ovarian tumors, BOTs are usually diagnosed in the early stages. They also tend to occur in younger ages and their long-term prognosis is significantly better. [3],[4] The gold standard treatment of BOTs is surgery. The surgical method should be determined according to patient's age, fertility status, and the stage and histopathological characteristics of the disease. Conservative surgical methods preserving the patient's fertility are preferred to conventional radical surgery because of a better prognosis and younger age. An accurate intraoperative histological diagnosis has a critical value in these patients, because they can be cured sufficiently with a conservative approach. [5] This is vitally important in order to apply the correct surgical management and to avoid over- or undertreatment. Although preoperative imaging methods and tumor markers are used to obtain knowledge about the characteristics of these tumors, intraoperative frozen section analysis is widely used to perform adequate surgery. However, the frozen section has been found to be a less reliable tool in the diagnosis of BOTs compared to benign and invasive epithelial ovarian tumors. [6],[7] In the current study, we investigate the diagnostic accuracy of the frozen section and the factors affecting the frozen section results in BOT patients. Materials and Methods A total of 82 histologically confirmed BOT patients, between January 1994 and June 2009, who had frozen section evaluation and regular follow-up were included in the study. Data has been obtained on the basis of patient files and pathology reports. The study was conducted as a retrospective cohort study. Patients with invasive ovarian tumors, BOT cases without frozen evaluation, and patients with incomplete file data were excluded. The clinicopathological characteristics, treatment methods, frozen section, permanent paraffin section results, and the factors possibly affecting the false frozen section results (age, histological type, mass dimension, location, characteristics of mass, capsule invasion, ascit presence preop. CA 125 level) were taken into consideration. 'Correct diagnosis' (borderline) was defined when the paraffin section result was the same as the frozen section result. When the frozen result was not borderline it was defined as a 'false diagnosis'. The term 'underdiagnosis' was used for a benign frozen result and 'overdiagnosis' was used for a malignant frozen section result. Conventional (complete) staging surgery included total abdominal hysterectomy with bilateral salpingo-oophorectomy (TAH-BSO), omentectomy, retroperitoneal lymph node dissection, and sampling peritoneal cytology. Any operation where the uterus and functional ovarian tissue remained at least in one ovary was defined as conservative (fertility preserving) surgery. Both groups of patients were included in a standard 10-year follow-up program. Three pathologists, experienced in gynecological pathology, evaluated the frozen section samples. Two sections were taken for sampling from the solitary or papillary structures of the tumors. When the tumors were bilateral, frozen sections were taken from both ovaries. For statistical analysis, the SPSS 17.0 for Windows statistical package program was used. Descriptive statistics and cross tables were carried out for evaluating data. The diagnostic rates, such as, accuracy, underdiagnosis, and overdiagnosis of the frozen section were estimated by accepting the paraffin section results as the gold standard. In order to investigate the factors associated with the false frozen section result, a chi-square test and multivariable logistic regression analysis were applied. The results were evaluated in the 95% reliability range and P < 0.05 was accepted as the statistical significance. Results The mean age was 40.16 ± 14.01 (range: 15 - 73), and 54.9% of the cases were found to be under 40. Histological distribution was as follows: 39 (47.5%) serous BOT, 35 (42,6%) mucinous BOT, four (4.9%) endometrioid BOT, and four (4.9%) mixed type BOT. 90.2% (74/82) of the cases were stage I. There were only two (2.5%) stage II and six (7.3%) stage III cases. The mean ovarian mass diameter was 14.11 cm (4 - 37 cm) (11.02 cm for serous tumors and 18.77 cm for mucinous tumors). In general, the bilaterality rate was 15.9% (13 / 82), and 92.3% (12 / 13) of the bilateral cases was serous BOT and only one case was mucinous. The mean preoperative CA 125 value was 118.11 IU / ml (2 - 678 IU / ml). It was 172 IU / ml, 39 IU / ml, and 53 IU / ml for serous, mucinous, and endometrioid type tumors, respectively. A high CA 125 level (> 35 IU / ml) was detected in 31 of the 74 cases with stage I, while it was observed in seven of the eight cases with further stages. Of the patients, 46,3% (38 / 82) had a high CA 125 level. The high CA 125 level was in 25 / 39 (64.1%) of the serous tumors, 9 / 35 (25.7%) of the mucinous tumors, 3 / 4 (75%) of the endometriod tumors, and 1 / 4 (25%) of the mixed tumors. Forty-two patients were treated with complete staging surgery and 40 patients were treated with fertility preserving surgery. Complete staging surgery was applied in 45.9% (34 / 74) of the stage I cases, and 100% (8 / 8) in further stages. A total of 25 patients underwent laparoscopic surgery initially, but five of them were completed by laparotomy. Frozen section evaluations revealed that 29.3% (24 / 82; underdiagnosis) of the tumors were benign, 69.5% (57/82) were borderline, and 1.2% (1 / 82; overdiagnosis) were malignant. Therefore, the accuracy rate of the frozen section evaluation for BOTs was 69.5%. This rate was 69% (27 / 39) for serous BOTs, and 65% (23 / 35) for mucinous BOTs. The factors predicting false frozen section results were primary ovarian tumor diamater (P = 0.005), solid / cystic status of the ovarian mass (P = 0.000), preoperative serum CA 125 level (P = 0.016), and intraoperative capsule status (intact or ruptured) of the mass (P = 0.049) [Table - 1]. In a multivariable logistic regression analysis, where the significant factors were evaluated in combination, the preoperative serum CA 125 level was only detected as a predictive factor [Table - 2]. Discussion In this study age, the histological type, FIGO stage, bilaterality, and serum CA 125 were found to be in accordance with the literature. [8],[9],[10],[11] Kolwijck et al., analyzed three studies and showed that high CA-125 values (> 35 U / mL) were determined in 53% of the BOT patients. Median CA 125 level was significantly higher in patients with serous (median, 59 U / mL) compared to those with mucinous (median, 25 U/mL) tumors. [10] In our study, 46,3% (38/82) of all patients had a high CA 125 level. In cases where the preoperative CA 125 value was ≤ 35 IU / ml, the rate of underdiagnosis was approximately 3.3 times higher than in cases with higher values (43.2% vs. 13.2%). As shown in [Table - 2], in the multivariable logistic regresion analysis, the CA 125 value was also the only predictive factor. On the other hand, there were limited data on the comparison of invasive and borderline ovarian tumors with respect to the serum CA 125 level. Hirai et al.'s study on the 146 stage 1A ovarian tumors including 61 BOTs and 85 invasive ovarian cancers showed that the CA 125 level was significantly higher in invasive cancer cases than that in BOTs. [12] For patients with a pelvic mass, it is wrong to make a diagnosis and surgical management only on the basis of the macroscopic characteristics of the mass. In other words, it is important and sometimes necessary to have intraoperative frozen section analysis. Frozen section examination was first applied in 1816, by De Remier, and was first used for intraoperative diagnosis by William Welsh. [13] It is widely used in surgery of suspicious ovarian masses. However, it should be kept in mind that the BOTs show the highest rate of false diagnosis with frozen section analysis. In benign and invasive ovarian tumors, the reported accuracy of the frozen section is quite high and is found to be between 90 - 96%. [14],[15] The sensitivity of the frozen section, to distinguish the benign and the malignant ovarian tumors, is 65 - 97%, and its specificity is 97 - 100%. [16] The mucinous BOTs have the lowest rate of accuracy with a frozen section. [17] In a study conducted by Pinto et al., the rate of accuracy with frozen section for ovarian tumors was 94%, with the rates of 98% for malignant tumors, 94% for benign tumors, and 78% for BOTs. [18] Yermez et al., reported 50% consistency between the frozen section and the final pathological results in the diagnosis of BOTs. [19] Tempfer et al., analyzed 317 BOT cases from three large studies and reported the sensitivity and PPV of the frozen section for BOT to be 71.1 and 84.3%; respectively. The consistency between the frozen section results and the final pathological diagnosis was 62.8% (199 / 317). [20] A study by Kayikcioglu et al., revealed a correlation of 72.7% between the frozen section results and the final pathological diagnosis. The rate of inconsistency for the serous types was 9% and for mucinous types it was 36.6%. [21] Puls et al., detected 10 cases, one stromal invasive (23%), in paraffin sections of 44 patients reported to havebe borderline with frozen section. Their study revealed that the rate of false diagnosis was higher in the mucinous types (33%) than in the serous types (13%). [22] Bige et al., reported that 18.2% of the cases defined as BOT by frozen results turned out to be malignant with the final pathological analysis. [23] On the basis of these results, we can conclude that the frozen section analysis has high rates of accuracy for distinguishing malignant and benign cases; however, it remains insufficient for distinguishing malignant and borderline. The gynecological surgeon should be aware that the intraoperative BOT diagnosis can change in favor of invasive tumors after surgical staging and paraffin section examination. If frozen section points to BOT in a woman with no concern about fertility, a proper surgical staging is necessary. [24] In a study in which the frozen and the paraffin sections were investigated by two groups of pathologists, one group comprised of experts in gynecological pathology and the other not in this field. It was observed that the paraffin section results were more consistent with the frozen section results in the group made up of experts in gynecological pathology. Therefore, the level of knowledge and experience of the pathologist is important in making a correct diagnosis. [22] Brun et al., also reported that the experience and expertise of the investigating pathologist is a determining factor for correct diagnosis besides the characteristics of the tumors. [25] In our study, we studied with three pathologists experienced in gynecological pathology and found the accuracy, underdiagnosis, and overdiagnosis rates to be 69.5, 29.3, and 1.2%; respectively. We suggest that this may explain our very low overdiagnosis rate (1.2%). In [Table - 3], we provide an overview of the literature concerning the accuracy, overdiagnosis, and underdiagnosis rates of the frozen section analysis in BOTs. Houck et al., reported the rates to be 10.7% for overdiagnosis and 29.3% for underdiagnosis. They noted that the rate of false diagnosis with a frozen section was higher for non-serous tumors. The most significant predictive factor for underdiagnosis was mucinous histology. [26] Tempfer et al., reported the rates of underdiagnosis and overdiagnosis as 28% (27 / 96) and 0%; respectively. The only independent predictive factor for underdiagnosis was the size of the ovarian mass (p = 0.04). [20] Kim et al., also reported larger tumor size in underdiagnosed patients (p = 0.021). [27] Li et al., detected the rate of underdiagnosis as 24.7%, and the predictors of underdiagnosis were tumor size and histology. However, in the multivariant analysis, only the tumor size was detected as a predictive factor. [28] In our study, as presented in [Table - 1], we detected low rates of underdiagnosis in a frozen section with the mass equal or larger than 5 cm (24 / 78). Solid or semisolid masses had a lower frequency of underdiagnosis (16 / 67; 23.9%) than pure cystic masses (8 / 15; 53.3%). In conclusion, the correct diagnosis to select less invasive surgical techniques and apply conservative surgical procedures, which preserve fertility, is crucial at pelvic mass operations. The intraoperative frozen section analysis may provide valuable information for the histological diagnosis and may also help to determine the type of management. However, the general diagnostic performance of the frozen section for BOTs is not satisfactory, with approximately 30% of underdiagnosis. In order to reduce the probability of false diagnosis, the frozen section analysis should be applied by experienced pathologists, who are experts in gynecological pathology, and all the possible predictive factors affecting false diagnosis should be carefully taken into consideration. References
Copyright 2011 - Journal of Cancer Research and Therapeutics The following images related to this document are available:Photo images[cr11113t3.jpg] [cr11113t1.jpg] [cr11113t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}