 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
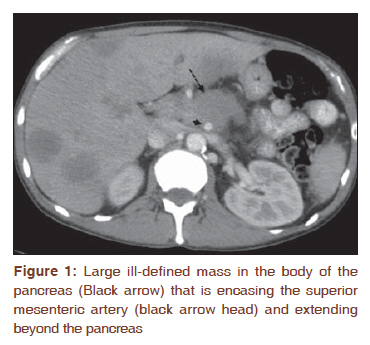
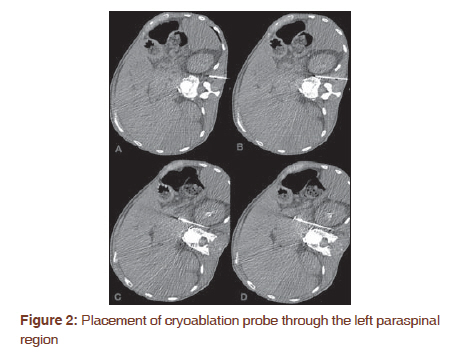
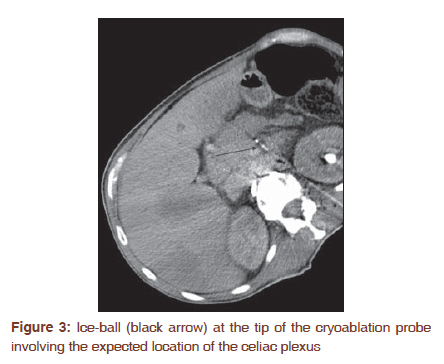
Journal of Cancer Research and Therapeutics, Vol. 7, No. 4, October-December, 2011, pp. 481-483 Brief Communication Percutaneous computed tomography guided cryoablation of the celiac plexus as an alternative treatment for intractable pain caused by pancreatic cancer Hooman Yarmohammadi1, Dean A Nakamoto1, Nami Azar1, Salim M Hayek2, John R Haaga1 1 Department of Diagnostic Radiology, University Hospitals Case Medical Center/Case Western Reserve University, Cleveland, USA Code Number: cr11125 DOI: 10.4103/0973-1482.92024 Abstract Computed Tomography (CT)-guided percutaneous cryoablation was performed in a 43-year-old patient with intractable epigastric abdominal pain caused by advanced adenocarcinoma of the pancreas and extensive celiac trunk involvement. Initial treatment with celiac plexus nerve neurolysis using local ethanol injection was unsuccessful. A 17-gauge 17-cm cryoablation probe (Galil Medical Inc. Plymouth Meeting, PA) was placed into the expected location of the celiac plexus through a left paraspinal approach under CT guidance and two cycles of freeze-thaw were performed. Patient's pain decreased from 10 of 10 (subjective pain scoring using a visual analog scale; VAS; 0-10) to 3. No post-procedure complication was observed. His pain has remained stable after 6 months of follow up. Percutaneous cryoablation appears to be an effective alternative to neurolytic celiac plexus block for palliative treatment of celiac plexus involvement. Further study with larger number of patients is needed to evaluate the safety and efficacy. Keywords: Celiac plexus, cryoablation, CT guided, neurolysis, pancreas cancer Introduction Multiple methods have been previously reported to be effective in relieving pain of celiac plexus involvement. Haaga et al. performed CT-guided bilateral and unilateral celiac ganglia block in patients with pain secondary to pancreatic cancer and reported satisfactory results. [1] Rykowski and Hilgier reported that unilateral transcrural celiac plexus neurolysis provides effective pain relief in patients with pancreatic cancer pain. [2] They performed neurolytic celiac plexus block (NCPB) using ethanol and were successful in 74% of the patients. [2] NCPB is effective only when a complete (four quadrant) spread of the neurolytic solution in the celiac area is obtained. [3] Therefore, in patients in whom the celiac area anatomy is altered by pancreatic tumor infiltration, complete spread of the neurolytic agent may be difficult and frequently impossible. [3],[4] Additionally, previous surgery or fibrosis secondary to radiation therapy can cause treatment failure. [4] We present a patient with advanced pancreatic cancer and intractable pain in whom percutaneous CT-guided cryoablation was performed for pain relief. To our best knowledge, this is the first report in which percutaneous CT-guided cryoablation has been used for celiac plexus block. Case Report Informed written consent was obtained. The patient, a 43-year-old gentleman, had initially presented with complaints of right upper quadrant pain and a 5-cm mass in the body of the pancreas was detected that encased the celiac and superior mesenteric artery origins [Figure - 1]. CT-guided biopsy of his liver lesions confirmed metastatic adenocarcinoma of the pancreas. Chemotherapy was initiated; however, his pain had worsened and at times he had been rating it as 10 of 10 (subjective pain scoring according to a visual analog scale; VAS; 0-10). A conventional CT-guided celiac plexus nerve block (complete four quadrants) using ethanol was performed. The patient's pain had not changed after 2 weeks post-injection and so it was concluded that nerve block was unsuccessful. Therefore, celiac plexus nerve block using cryoablation was suggested. The patient was placed in the right lateral decubitus position. The expected location of the celiac plexus was localized under CT guidance. Approximately 100 ml of isoversol was injected as two separate 50-ml boluses to localize the celiac axis. Lidocaine was used for local anesthesia. Left paraspinal approach was utilized, and a Chiba needle was advanced to the expected location of the celiac axis. Next, a 17-gauge 17-cm ice sphere cryoablation probe (Galil Medical Inc. Plymouth Meeting, PA) was placed into the expected location of the celiac plexus through left paraspinal approach [Figure - 2A-D]. The patient then underwent cryoablation with a 15-minute freeze period followed by a 5-minute active thaw. A second 10-minute freeze was then performed, followed by a second active thaw. An Ice-ball measuring 10 × 19 mm was formed at the tip of the probe [Figure - 3]. No immediate post-procedure complications were detected. The patient reported improvement in his pain, from VAS score of 8-9/10 to 5-6/10 on the CT table and during the procedure. The day following his procedure, the patient's pain had decreased to 3-4 of 10. His abdominal pain remained 3 of 10 at the 6-month follow-up. Discussion Currently, the WHO policy in treating cancer pain, introduced in 1986, is a sequential three-step Analgesic Ladder (NSAID-opioids). [5] Interventional modalities are suggested as the fourth step of the ladder; however, this has not generated a clear consensus. [6] Multiple studies have demonstrated that neuroablative procedures improved quality of life in patients with cancer pain when compared with oral analgesics. [7] With the dramatic improvement in procedural and imaging techniques, there is progressive tendency toward interventional techniques. Whether these should move to the first step of the WHO ladder is a question that should be answered in the near future. [6] If non-interventional methods of pain control fail, NCPB is appropriate to achieve the optimal pain relief in all cases of pancreatic cancer. However, if NCPB also fails, then there are a few other minimally invasive treatments available. [2] Thoracoscopic splanchnicectomy has been suggested to offer more sustained long-term pain relief and appears to be with few or no complications. [8],[9] Prasad et al. and Kordiak et al. utilized it as a palliative procedure for pain relief in patients with pancreas cancer and achieved satisfactory results. [8],[9] Rykowski and Hilgier reported that larger tumors, tumors in the body and/or tail of the pancreas, and in tumors that have caused anatomical distortion, NCPB will be associated with higher chance of failure. [2] Our patient presented in an advanced stage of pancreatic cancer with extensive involvement of the celiac plexus and distortion of the anatomy; hence, we speculated that these were the reasons for an unsuccessful NCPB. Cryoablation in combination with CT guidance allows the interventionist to visualize the ice-ball formation during the procedure. Cryoablation causes sudden and progressive damage to the pancreatic cells in the post-cryosurgical zone secondary to aseptic cryonecrosis and cryoapoptosis of vital normal tissue. [10] The low temperature induced by the cryoablation produces vascular capillary changes, circulatory stagnation, and consequently has anti-angiogenesis characteristics. [10] Recently, cryoablation has been utilized in patients with unresectable pancreatic cancer and has shown to be safe and effective. [11],[12] Kovach et al. performed intraoperative cryosurgery on 9 patients with unresectable pancreatic cancer. [11] No mortality or major complication was detected and following the treatment, all patients experienced alleviation of their pain. Li et al. performed palliative bypass surgery with and without cryoablation in 142 patients with unresectable pancreatic cancer and demonstrated that although the size of the tumor decreased, the overall 5-year survival rate did not increase. [13] In order for cryoablation to be effective, temperatures at or below -40°C is required. It is believed that in order to achieve adequate ablation, 1-cm ice-ball extension beyond the tumor borders is required. [14] In our study, we estimated the size of the mass surrounding the plexus approximately 15 × 15 mm. We set our goal to produce an ice-ball with the size of 20 × 20 mm in order to obtain satisfactory result. The celiac plexus is usually not visible and therefore we placed the 17 G cryoablation probes in the center of the mass, between the celiac axis and superior mesenteric artery origin while avoiding the aorta. The ice-ball formation was slightly smaller than expected. Some of these may be due to perfusion-mediated tissue heat dissipation effect from the aorta and other vessels. We were not sure if the location of the probes was the most optimal location, but the results seem to show it was sufficient. It is quite clear that the heat convection from the flowing aorta was more than enough to protect the aorta. In conclusion, percutaneous cryoablation appears to be an effective alternative to NCPB for palliative treatment of celiac plexus involvement. References
Copyright 2011 - Journal of Cancer Research and Therapeutics The following images related to this document are available:Photo images[cr11125f3.jpg] [cr11125f1.jpg] [cr11125f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}