 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
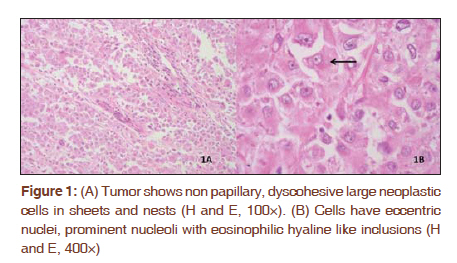
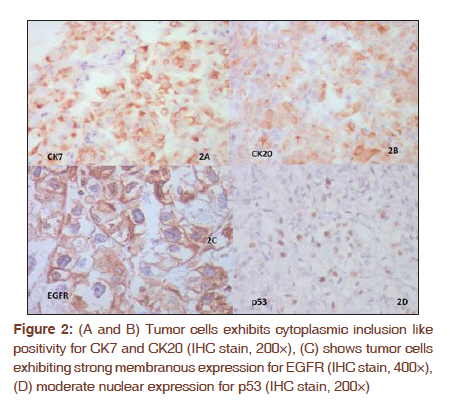
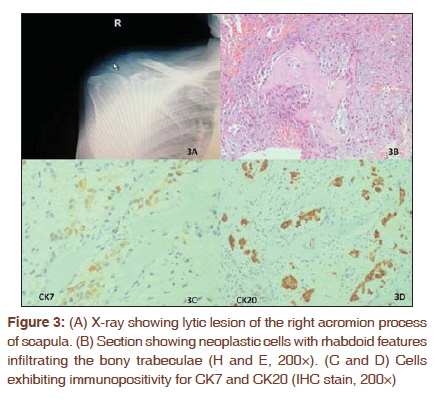
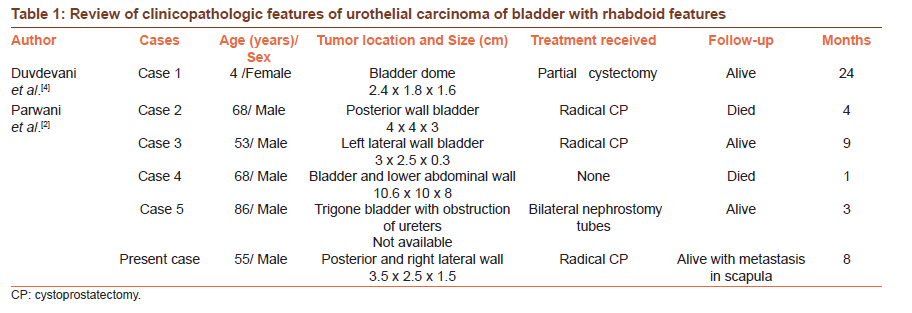
Journal of Cancer Research and Therapeutics, Vol. 7, No. 4, October-December, 2011, pp. 486-488 Letter to the Editor - Documenting a Case Urothelial carcinoma of bladder having rhabdoid differentiation with isolated scapular metastasis Sunil Pasricha, Ather Hafiz, Jatin S Gandhi, Anurag Mehta Department of Pathology, Rajiv Gandhi Cancer Institute and Research Centre, New Delhi, India Code Number: cr11127 DOI: 10.4103/0973-1482.92008 Sir, Rhabdoid tumor was originally described by Beckwith and Palmer as a highly malignant renal tumor of childhood. Tumors with similar features have been documented in extra renal sites and also in adults. The histogenesis of these tumors is uncertain, however, electron microscopic studies in most cases have revealed cytoplasmic aggregates of intermediate filaments. Tumors with rhabdoid phenotype are associated with an aggressive clinical course. [1],[2] Urothelial carcinomas of bladder with rhabdoid differentiation are very rare and only handful of cases have been described in the literature. [1],[2],[3],[4],[5] We present a case of urothelial carcinoma of bladder with prominent rhabdoid features in adult male with unusual distant bone metastasis to the acromian. A 55-year-old male, known case of diabetes mellitus and hypertension with past history of coronary artery bypass graft presented with history of hematuria for four to five months. Routine laboratory investigations were normal. Cystoscopic biopsy was performed which revealed high grade urothelial carcinoma infiltrating into the muscularis propria which eventually led to radical cystoprostectomy with ileal conduit. Grossly, the tumor measured 3.5 x 2.5 x 1.5 cm predominantly involving posterior and right lateral wall infiltrating upto the perivesical fat. Rest of the structures were grossly unremarkable. Microscopic examination revealed high grade urothelial carcinoma with eccentric hyperchromatic nucleus, prominent eosinophilic nucleoli, and moderate to abundant eosinophilic cytoplasm with many cells showing intracytoplasmic round hyaline-like inclusions [Figure - 1]. The tumor was infiltrating as nests and sheets through the muscularis propria into the perivesical fat. Immunohistochemical (IHC) study showed tumor cells were strongly positive for cytokeratin (CK), CK7, CK20, and focally for vimentin. The inclusion like positivity was evident in many cells [Figure - 2a,b]. Epidermal growth factor receptor (EGFR) expression and ki-67 index was high, whereas p53 positivity was moderate [Figure - 2c,d]. The tumor cells and inclusions were however negative for desmin. In view of morphological and IHC findings, a final diagnosis of high grade urothelial carcinoma with rhabdoid differentiation was established. Lymphovascular permeation was indeterminate. An incidental microscopic finding of prostatic adencarcinoma was found with Gleason's score of 3+3 = 6, involving periurethral region of lower lobe. Bilateral pelvic lymph node dissection did not reveal metastatic deposit in any of the twenty lymph nodes dissected. Patient also received adjuvant chemotherapy. Till eight months of follow-up patient was doing well but then developed pain in the right shoulder region. Radiological studies revealed lytic lesion in right acromian process of the scapula. A trucut biopsy was performed which showed metastatic carcinoma with morphology and immunohistochemical profile similar to that of primary urothelial carcinoma with rhabdoid differentiation [Figure - 3]. Rhabdoid tumor was originally described as a distinctive, highly malignant neoplasm of the infant kidney. Though initially regarded as variant of wilms' tumor, it was subsequently shown to be a distinct clinicopathological entity lacking features of myogenous differentiation. [1],[4],[6] Tumors with similar morphology have been reported in extrarenal sites and also in adults. [1] Malignant tumors with rhabdoid features in adults in extrarenal locations are considered to be phenotypic variants and have been described in multiple sites including the extremities, brain, liver, mediastinum, orbit, heart and others and is now accepted as a discrete entity. [2] The diagnosis of extrarenal rhabdoid tumors is nearly always based on the morphologic resemblance of the tumor cells to those of "classic" pattern of malignant rhabdoid tumor of kidney featuring hyperchromatic eccentric nuclei, large nucleoli and abundant eosinophilic cytoplasm containing inclusions. Ultrastructural studies have confirmed that the eosinophilic body corresponds to whorls of intermediate filaments. IHC findings usually demonstrate reactivity to CK, vimentin and desmin. [1],[2],[6] A review of clinicopathologic features of urothelial carcinoma of bladder with rhabdoid features is summarized in [Table - 1]. Parwani et al., has described four cases of urothelial carcinomas of urinary bladder with rhabdoid features in adults. [2] Two of these died early and two were alive on follow-up period for 3 months and 9 months. In the presented case, the patient developed distant metastasis in the form of scapular involvement after eight months. The morphological and IHC features in the metastatic site corresponded to high grade urothelial carcinoma with rhabdoid differentiation. EGFR expression and ki-67 index was high in the primary bladder tumor, which corresponded to their increased expression with grade, stage, and non papillary configuration. The p53 positivity was moderate, which is associated with grade, stage, and papillary status. [7] Bone metastasis from urinary bladder carcinoma are not rare and the most common site is the spine. Distant bone metastasis to the acromian from the urothelial carcinoma of bladder is extremely rare and to the best of our knowledge this is the second case in the literature. Forte et al., described the first case metastasising to the acromian process.[8] Weizer et al., has described a metastatic transitional cell carcinoma of the urinary bladder to the soft tissue of the shoulder girdle. [9] Tumor with rhabdoid phenotype are associated with an aggressive clinical course. [1],[5] Many extra renal rhabdoid tumors have proven lethal but this phenomenon is not universal. [6] Few authors supported the fact that extra renal rhabdoid tumors represent a diverse phenotype rather than the distinct clinicopathological entity of true rhabdoid tumor of childhood. [1] In conclusion, the clinicopathological features of the presented case supports the aggressive clinical behaviour of urothelial carcinoma with rhabdoid differentiation with unusual sites for metastasis. This rare entity in adults represents a rare phenotypic variant of urothelial carcinoma or a distinct clinicopathological entity is uncertain due to limited number of cases in the literature. Distant bone metastasis to the acromian is exceedingly rare, however, should be kept in mind when patient presents with shoulder pain. References
Copyright 2011 - Journal of Cancer Research and Therapeutics The following images related to this document are available:Photo images[cr11127f3.jpg] [cr11127f2.jpg] [cr11127f1.jpg] [cr11127t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}