 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
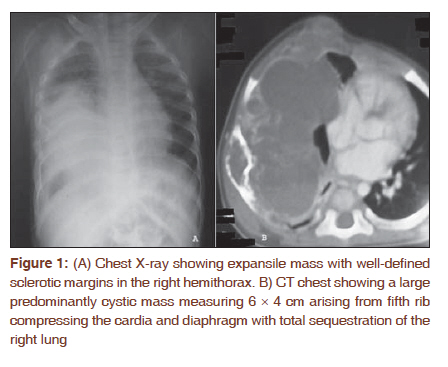
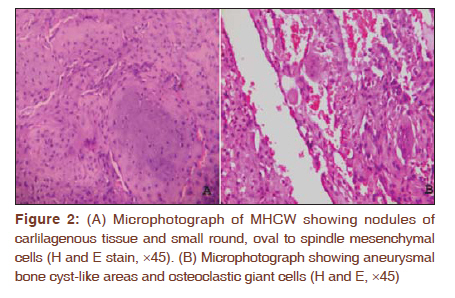
Journal of Cancer Research and Therapeutics, Vol. 7, No. 4, October-December, 2011, pp. 496-498 Letter to the Editor - Documenting a Case Mesenchymal hamartoma of the chest wall- mimicker of malignancy Sunil Kumar Yeshvanth1, Veena Shivamurthy1, Channappa Patil2, Sandeep Rai3, Kishan Prasad H Lakshminarayana1, Jagadish H Makannavar1 1 Department of Pathology, K. S. Hegde Medical Academy of Nitte University, Deralakatte, Mangalore, Karnataka, India Code Number: cr11131 DOI: 10.4103/0973-1482.92017 Sir, Mesenchymal hamartoma of the chest wall (MHCW) occurs as intraosseous expansile mass involving the ribs typically present at birth or in early infancy. [1] The incidence is about 0.03% among primary bone tumors with male predominance, and appropriately 100 cases have been reported. The distinction between this benign tumor and malignant tumors like well-differentiated chondrosarcoma is seldom clear cut. [1] The aggressive clinical presentation, radiological features, and histological features like actively proliferating fibroblastic and chondroid elements can be mistaken for malignant process. [1] We present a case of 7-month-old female baby with slowly growing chest wall swelling since birth, previously evaluated and diagnosed as malignant tumor in a local hospital, on further evaluation in our hospital found to have MHCW. The patient was treated with thoracotomy and en bloc excision with no evidence of recurrence or complications seen on 2 years follow-up. A 7-month-old female baby presented with history of gradually progressive chest wall swelling since birth with recent onset of breathlessness. Obstetric and developmental history was uneventful. She was evaluated in local hospital and diagnosed to have immature teratoma of the chest wall, referred to our hospital for further management. On examination, baby had a firm, nontender, nonmobile, nonflunctuant swelling measuring 3 × 4 cm on the right upper chest wall. All hematological and biochemical parameters were within normal limits. Chest X-ray showed expansile mass with well-defined sclerotic margins in the right hemithorax [Figure - 1A]. Computerized tomography (CT) revealed a large predominantly cystic mass measuring 6 × 4 cm arising from fifth rib compressing the cardia and diaphragm with total collapse of the right lung [Figure - 1B]. A biopsy was performed and microscopy revealed nodules of carlilagenous tissue, small round, oval to spindle mesenchymal cells, aneurysmal bone cyst-like areas and osteoclastic giant cells [Figure - 2A,B]. A final diagnosis of mesenchymal hamartoma of the chest wall was made. Oncologist deferred the chemotherapy treatment, and thoracotomy with en bloc excision of the tumor was performed. Diaphragm and pericardium were free from the tumor and the right lung expanded well after the surgery. The patient is doing well 2 years after treatment without any recurrence or complications. MHCW is a very rare benign tumor of bone which was first described by Nash and Stout in 1961. [2] McLeod and Dahlin coined the term hamartoma of the chest wall; however, many authors coined in different names like mesenchymal, vascular, cartilaginous, and chondromatous hamartoma, whereas the preferred term is mesenchymal hamartoma of the chest wall. [2],[3] The 80% of cases occur prenatally or within first 6 months of life and are usually solitary, but bilaterality or multicentricity also rarely occur. [3],[4] Typically the lesion appears as a hard, immobile, subcutaneous, and extrapleural chest wall mass with deformed ribs. Respiratory distress and ventilator dependence may occur even in term or near-term newborns. [2] Mesenchymal hamartoma is not a true neoplasm, but rather they are hamartomas with focal overgrowth of normal skeletal elements with no propensity for invasion or metastasis. Plain X-ray shows expansile mass with well-defined sclerotic margins with secondary aneurysmal bone cysts and popcorn-like speckled calcifications. [2],[3],[5] CT scan is a better modality which helps to determine the site of origin, tumor density, enlargement, and effect on adjacent structures. [5] Prenatal diagnosis is possible by ultrasonography, but most are diagnosed postnatally. Radiologically, MHCW can be confused with malignant tumors like congenital neuroblastoma, Ewing's sarcoma, and malignant teratoma. [5] The definitive diagnosis is established only by histopathological examination. [5] Grossly, they are well circumscribed comprising both cystic and solid areas, microscopically having small round, oval, or spindle mesenchymal cells, osteoclastic giant cells, fragments of hyaline cartilage, and aneurysmal bone cyst-like changes. [2] Immunohistochemically, chondrocytes stain for S-100 protein and factor VIII highlighting the blood vessels. The differential diagnosis includes well-differentiated chondrosarcoma, aneurysmal bone cyst (ABC), chondroma, osteosarcoma, langerhans cell histiocytosis (LCH), and osteochondromas. [2],[3] Chondrosarcomas occur at the periphery of the ribs and grow rapidly with presence of atypical mitosis, hence differentiated from MHCW. In the series of Ayala et al., [5] one case of MHCW was misdiagnosed as chondrosarcoma. [3] ABC-like areas were seen only focally, and the presence of cartilaginous tissue with mesenchymal cells ruled out the possibility of primary ABC. Tumors with such huge size, cystic change, and hypercellularity with presence of mesenchymal cells are usually not seen in chondromas. Osteosarcoma, LCH, and osteochondromas can be ruled out by the absence of pleomorphic spindle cells with malignant osteoid, atypical histiocytes with longitudinal grooves in the background of eosinophils and osteocartilagenous cap with marrow tissue, respectively. Malignant transformation in MHCW is very rare. [6] Symptomatic patients having cardiorespiratory compromise or causing deformity are best treated by complete resection and prognosis is very good. [3] However, MHCW stops growing within the first year of life and some patients may have an excellent outcome with conservative treatment alone. [2],[3] Spontaneous regression has been observed in children even with bilateral involvement supporting the concept that conservative management is appropriate for asymptomatic children. Chemotherapy as well as radiation is not indicated in the treatment of MHCW. The most important postsurgical complication is scoliosis seen in 20% of patients. [2] We hereby conclude that although these tumors are rare and they look aggressive both radiologically and microscopically, it is important to be aware of this condition, so that unnecessary overdiagnosis and aggressive treatment with chemotherapy and radiotherapy can be avoided for the fast recovery of the patient when managed with surgery alone. Acknowledgement We kindly acknowledge Dr Jayaprakash Shetty K, Professor and Head of Pathology for his valuable suggestions and guidance. References
Copyright 2011 - Journal of Cancer Research and Therapeutics The following images related to this document are available:Photo images[cr11131f2.jpg] [cr11131f1.jpg] |
| |||||||||

{kind=link}
{kind=link}