 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Dermatology, Venereology & Leprology, Vol. 69, No. 3, May-June, 2003, pp. 209-211 Study Diltiazem vs. nifedipine in chilblains: A clinical trial A. K. Patra, A. L. Das, P. Ramadasan Department of Dermatology, STD & Leprosy, Military Hospital, Agra, India.
Abstract Background: The treatment of chilblains remains unsatisfactory.
Nifedipine in higher doses remains the mainstay of treatment. Aims: To
compare the efficacy of diltiazem with that of nifedipine, and to determine
the efficacy of nifedipine in lower doses, 36 chilblains cases were studied. Material
and Methods: Group A (12 patients) was treated with diltiazem 60 mg thrice
daily, and Group B (24 patients) with 10 mg nifedipine thrice daily till complete
relief and then maintained on a sustained release preparation of nifedipine
20 mg twice daily. Results: Two patients in Group A showed complete
relief in 7 days, and 3 patients in about 21 days, but in 7 cases there was
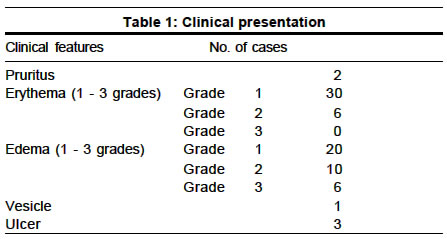
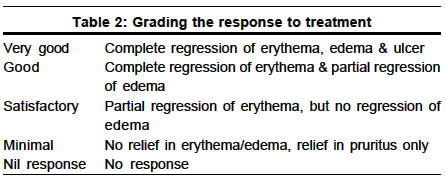
little or no response. In group B, 21 cases showed 80-90% relief by the fourteenth Key words: Calcium channel blockers Introduction Dowd et al1 in 1986 first established the use of nifedipine in the treatment of chilblains or perniosis, in the dosage of 20 mg of sustained release preparation of nifedipine three times a day over a 6-week period. This was later confirmed by Rustin et al2 in 1989 in a larger series over a prolonged period, both for treatment and for prophylaxis. The present trial was conducted to compare the efficacy of diltiazem, a newer calcium channel blocker, with that of nifedipine, and to determine the efficacy of nifedipine in lower pharmacological dosages, since Indians are more thinly built than their Western counterparts. Material and Methods Thirty-six patients participated in this trial, which was conducted over three winter seasons, from 1999 to 2001, in Northern and Central India. All patients were clinically diagnosed as chilblains. Their blood pressure was measured, and a routine hemogram and urinalysis performed. They were divided into two groups at random. Group A was given diltiazem 60 mg three times a day. Group B was given 10 mg of nifedipine (plain) thrice a day till complete relief and then maintained on a sustained release preparation of nifedipine 20 mg twice a day: Some of the patients, being serving soldiers, were admitted for daily follow up and record of blood pressure, while others were advised to record their basal blood pressure wherever possible. All were advised to report in case of adverse reactions like flushing, headache or dizziness. Patients of both groups were reviewed on the 3rd, 7th, 14th and 21st days, and then once every 7th day until complete remission. Results The clinical features of chilblains ranged from pruritus to erythema and edema to vesicles and ulceration (Table 1). The hands and feet were affected in 35 patients, and the face and ears in 1. All patients were normotensive with normal hemogram and urinalysis. Group A included 12 averagely built adults (M:F = 5:7). Response to treatment was graded into very good, good, satisfactory, minimal and no response as shown in Table 2. In 2 cases complete relief was noted within 7 days, while in 3 cases response was first observed around the 7th day and complete relief took about 21 days. However, in 7 cases there was no response after 7-10 days and they were switched over to Group B (Table 3). Group B included 25 averagely built adults (M:F =18:7). They were initially given nifedipine 10 mg twice a day and reviewed after 3 days for any side effects. Subsequently, nifedipine was given thrice a day. Review on the 7th day showed good clinical response, which was sustained till about 14 days, when there was 80-90% relief in most cases. After the 14th day all patients were treated with 20 mg of a sustained release preparation of nifedipine twice a day till complete relief. The spectrum of response ranged from relief in pruritus by about the 3rd day, erythema by about the 7th day and disappearance of edema by about the 14th day. A few cases with severe edema and ulceration took another 5-7 days for complete recovery. Response was seen earlier on the hands than over the feet (Table 2). All patients tolerated drugs well, except for one who complained of dizziness immediately after taking nifedipine. This patient was given a capsule of nifedipine under observation, but again developed dizziness and hypotension. He was then excluded from the study. Discussion Chilblains are the result of an abnormal reaction to cold and are usually localized to acral sites. The lesions are often itchy, and usually tender, erythematous, and inflammatory, and may blister or ulcerate. Although many factors have been implicated in the etiology, varying from genetic to hormonal to increase in nerve bundles, yet one thing is constant: a persistent cold induced constriction of the large cutaneous arterioles and persistent dilatation of the smaller, more superficial vessels.1 Histopathologically, chilblains are characterized by edema of the papillary dermis, a perivascular lymphocytic infiltrate, and thickening of the blood vessel walls with intimal proliferation leading to obliteration of vascular lumen. They are more common in women;4 however in our study the M:F ratio was 23:14, probably because most of our patients were soldiers, serving at higher altitudes in extreme cold climates out in the open. The treatment of chilblains remains unsatisfactory. Nifedipine
and, to a lesser extent, diltiazem,3 both calcium channel blockers,
are reported to be effective. They modify calcium entry into cells by interacting
with specific binding sites on the 6. In our study nifedipine was used in a lower dosage than the 60 mg of a sustained release preparation of nifedipine used by Rustin et al2 since Indian subjects have a smaller frame/built and body weight. The clinical response was comparable to that in earlier studies of Rustin et al2 and Dowd et al.3 Moreover, this regimen causes fewer side effects, has better compliance and is cheaper. In the diltiazem group, no response was seen in 7 cases, poor response in 3 cases, and good clinical response was seen only in two cases. We conclude that nifedipine remains the drug of choice in chilblains but can be used in a smaller dosage in the Indian population. Diltiazem is less effective in the conventional dose and we propose to conduct further studies with a higher dosage in a larger group of patients.
References
Copyright 2003 - Indian Journal of Dermatology, Venereology & Leprology. Free full text also available from: http://www.ijdvl.com The following images related to this document are available:Photo images[dv03004t1.jpg] [dv03004t2.jpg] [dv03004t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}