 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Dermatology, Venereology & Leprology, Vol. 69, No. 3, May-June, 2003, pp. 212-213 Study A comparative study of PUVASOL therapy in lichen planus Lata Sharma, M. K. Mishra Department of Dermatology & Venereology, Institute of Medical Sciences,
Banaras Hindu University, Varanasi, U.P., India.
Code Number: dv03005 ABSTRACT Background: PUVA therapy is reported to be effective in lichen planus. However, PUVASOL therapy is more easily available in India. Aim: To carry out a three way open comparison of oral PUVASOL therapy with oral metronidazole and with the conventional oral antihistamine plus topical steroid therapy. Material and Methods: Seventy-five cases of lichen planus were studied for 12 weeks with three different modalities: 1. Oral metronidazole and topical emollient cream, 2. Oral PUVASOL and topical emollient cream, and 3. Oral cetirizine and topical betamethasone dipropionate cream. Lesions were assessed before starting the treatment and after every 4 weeks. Results: Seventy patients completed the trial. Statistical analysis showed that therapy 1 was less effective than 2 and 3, which were found to be equally effective. Conclusion: It is concluded that PUVASOL therapy is a useful alternative to conventional therapy in lichen planus in our country where sunlight is available in plenty. Key Words: PUVASOL, Metronidazole, Cetirizine, Emollients, Photochemotherapy INTRODUCTION A topical steroid with an oral antihistaminie is the conventional treatment of lichen planus (LP).1 Metronidazole 250 mg thrice daily has been found to be effective in 4 out of 7 patients by Asher and Yahav in 1995.2 Response was also described with psoralens and ultraviolet light (PUVA) in 8 out of 10 cases by Gonzalez et al in 1984.3 In our country, photochemotherapy with solar radiation (PUVASOL) has been found to be effective and a cheaper alternative to PUVA in vitiligo, psoriasis and alopecia areata.4-6 Hence an open comparative evaluation of these therapies was done. MATERIAL AND METHODS Seventy-five adult patients of LP attending the dermatology OPD were selected. Patients suffering from amoebiasis, trichomoniasis, systemic illness, LP localized to mucosae or nails, or those treated for LP within the last 4 weeks, were excluded. Details of symptoms with duration and examination for site, number, type of LP lesions and distribution were recorded. Investigations done were: hemoglobin, total and differential count, urea, sugar, urine microscopy or culture to exclude infections, and stool examination for ova and cyst. Consecutive patients were advised three different therapies:
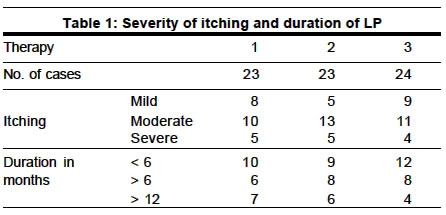
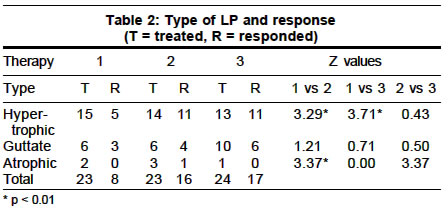
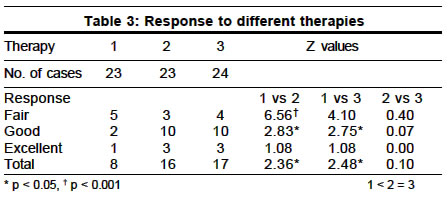
Lesions were assessed before starting the treatment and after every 4 weeks and response was graded as fair (mild decrease in symptoms, lesion size and number), good (moderate decrease in symptoms, lesion size and number), excellent (symptoms and lesions disappeared), or nil (no change in symptoms, lesion size and number or increase in symptoms, lesion size and number). RESULTS Thirty-four males and 36 females completed the trial. Their mean age and standard deviations were 33.71 and 11.42 respectively. The therapy groups were statistically comparable according to age and sex. Most of the patients showed moderate itching and duration up to 6 months (Table 1). The response to therapy varied with the type of LP. In the atrophic type, PUVASOL therapy was more effective than the other two. In the guttate type the response was similar with all the three therapies. In the hypertrophic type the response to therapies 2 and 3 were similar and better than therapy 1 (Table 2). Therapy 2 was superior to therapy 1 irrespective of the duration of LP and therapy 3 was more effective than therapy 1 in LP of more than 6 months' duration. More responded to therapies 2 and 3 as compared to therapy 1 (Table 3). Comparison of Z values showed that the response to therapies 2 and 3 was similar and was greater than therapy 1 statistically. Some side effects were also observed during the trial: in therapy 1, metallic taste in 3 cases and nausea in 2 cases; in therapy 2, nausea and sunburn in 1 case each; in therapy 3, striae at the site of application of steroid cream in one case. DISCUSSION Repeated and controlled phototoxic reactions act either by suppression of DNA synthesis and cell division7 or by direct ablative action on lymphocytes.8 In the present study, PUVASOL therapy showed a greater degree of improvement than metronidazole in lower doses2 and with fewer side effects. Its effectiveness was similar to conventional therapy. Therefore it can be used as an alternative therapy for cases of LP in our country where sufficient sunlight is available. REFERENCES
Copyright 2003 - Indian Journal of Dermatology, Venereology & Leprology. Free full text also available from: http://www.ijdvl.com The following images related to this document are available:Photo images[dv03005t2.jpg] [dv03005t3.jpg] [dv03005t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}