 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Dermatology, Venereology & Leprology, Vol. 69, No. 3, May-June, 2003, pp. 217-219 Study Therapeutic efficacy of intralesional triamcinolone acetonide versus intralesional triamcinolone acetonide plus lincomycin in the treatment of nodulocystic acne B. B. Mahajan, Geeta Garg Department of Dermatology, Govt. Medical College, Faridkot, Punjab, India.
Code Number: dv03007 Abstract Background: Intralesional triamcinolone is an established therapy for cysts of acne. However, intralesional antibacterials have not been used earlier. Aim: To compare the efficacy of intralesional triamcinolone with that of a combination of intralesional lincomycin and intralesional triamcinolone in nodulocystic acne. Material and Methods: Ten patients of nodulocystic were injected with intralesional triamcinolone acetonide (2.5 mg/ml), while nine patients were given lincomycin hydrochloride (75 mg/ml) in addition to the intralesional triamcinolone. They were followed up 48 hrs, one week and one month later. Results: At one week, 7 patients (70%) treated with injection triamcinolone showed 66% improvement, whereas all 9 (100%) patients treated with lincomycin and triamcinolone showed 100% improvement which was stable at one month. Conclusion: A combination of intralesional triamcinolone and lincomycin is superior to intralesional triamcinolone alone in the treatment of nodulocystic lesions of acne. Key Words: Nodulocystic acne, Intralesional triamcinolone, Lincomycin Introduction Nodulocystic acne may result in deep seated scars. Intralesional steroid injections may produce dramatic flattening of most acne nodules in 48-72 hours. They are commonly used when topical or oral therapy is not completely effective or when a more rapid response is necessary. This pilot study was undertaken to evaluate and compare the efficacy of intralesional triamcinolone acetonide versus intralesional triamcinolone acetonide plus lincomycin hydrochloride in nodulocystic acne.
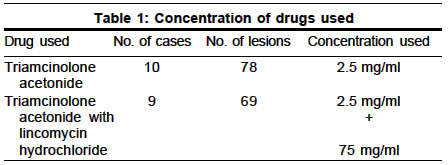
Material and Methods Nineteen clinically diagnosed patients with nodulocystic acne were enrolled in this study. Ten of them were given intralesional injections of triamcinolone acetonide, whereas nine were given intralesional triamcinolone acetonide plus lincomycin hydrochloride. The skin overlying the cyst was surgically prepared with povidone iodine. It was stabilized with the left hand and pierced at the most dependent point with a 26-gauge needle attached to a syringe. The needle was advanced till it met resistance (the cyst wall) which on further pressure suddenly yielded a feeling of give away, indicating that one had entered the cyst cavity. As acne cysts vary in size, the volume of injected material and hence the total dose was tailored to individual lesions. A cyst measuring 1 sq. cm. in size was injected with 0.1 ml of the drug, approximately the amount needed to blanch its surface. The concentration of triamcinolone acetonide was 2.5 mg/ml (made by diluting triamcinolone acetonide 10 mg/ml with water) and that of lincomycin hydrochloride was 75 mg/ml (made by diluting lincomycin hydrochloride 300 mg/ml with water) (Table 1). All the patients were examined after 48 hours, one week and one month. The response of an individual cyst was evaluated by using a 0-3 scale:
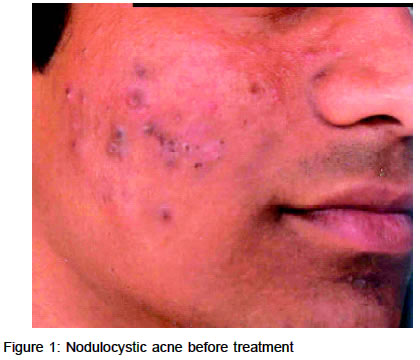
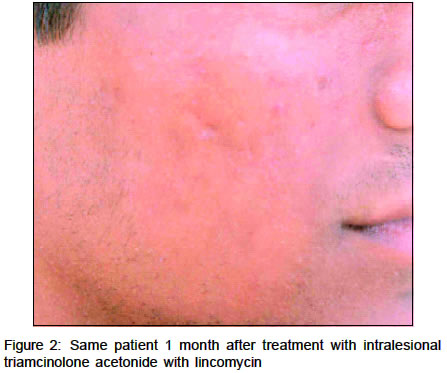
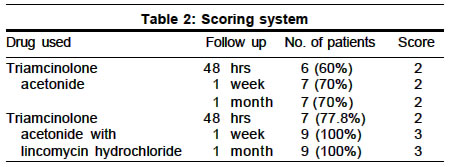
Results Of the 19 patients, 11 were male and 8 female. Their ages ranged from 16 years to 29 years, with a mean age of 22 years. The total number of lesions per patient selected for intralesional injections varied from 8 to12. Six (60%) of the ten patients injected with triamcinolone acetonide alone showed scale 2 improvement (i.e. 66%) after 48 hours, while seven (70%) patients showed improvement after 1 week (i.e. scale 2). This improvement remained stable at one month follow up (Figures 1 & 2). Seven (77.8%) patients of the nine who were given triamcinolone acetonide mixed with lincomycin hydrochloride showed scale 2 improvement (i.e. 66%) after 48 hours. All nine (100%) cases showed scale 3 improvement (i.e. 100%) after 1 week and this was sustained at one month follow up (Table 2). Discussion Intralesional injections of corticosteroid have been commonly used for the last 40 years, but there are not many reports of their effectiveness for nodulocystic acne. As a rule, concentrations of more than 5 mg/ml of triamcinolone acetonide are not used for intralesional injections because of the risk of atrophy.2 As triamcinolone acetonide is a long acting steroid, we believe that the drug remained in situ long enough to produce a substantial anti-inflammatory effect. Lincomycin hydrochloride, when used in combination with triamcinolone acetonide, not only acts as an antibacterial but possibly also as an immunomodulator. We do not believe that any improvement was due to the systemic effects of triamcinolone since we did not exceed a total dose of 5 mg ml in any patient. Potter, when using triamcinolone acetonide 5 mg/ml for intralesional injections, found that a total dose of 20 mg produce adrenal suppression.3 The tetracyclines, minocycline and doxycycline, besides their anti-infective action, exhibit potent immunomodulating properties, viz. inhibition of T cell proliferation and granuloma formation in vitro.4-6 In this study, intralesional injections of lincomycin hydrochloride (75 mg ml) with triamcinolone acetonide (2.5 mg/ ml) resulted in healing of all nodulocystic lesions of acne within 48 hours to 1 week. The effectiveness of the combination therapy may be due not only to the anti-inflammatory effect of steroids and the antibacterial action of lincomycin but also to the immunomodulatory actions of lincomycin. Further studies are required to determine the lowest concentrations of triamcinolone acetonide and lincomycin hydrochloride as a treatment modality in nodulocystic acne. References
Copyright 2003 - Indian Journal of Dermatology, Venereology & Leprology. Free full text also available from: http://www.ijdvl.com The following images related to this document are available:Photo images[dv03007t2.jpg] [dv03007f2.jpg] [dv03007f1.jpg] [dv03007t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}