 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Dermatology, Venereology & Leprology, Vol. 69, No. 3, May-June, 2003, pp. 220-222 Case Report Ichthyosiform sarcoidosis following chemotherapy of Hodgkin's disease M. P. S. Sawhney, Y. K. Sharma, V. Gera, *S. Jetley Department of Dermatology and STD and *Department of Pathology, Command Hospital,
Pune-411040, India.
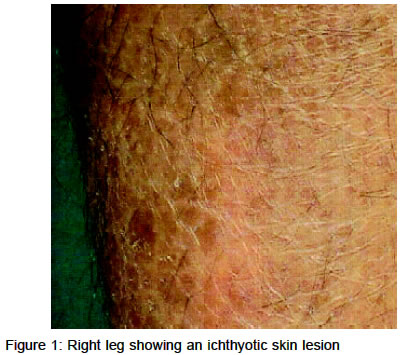
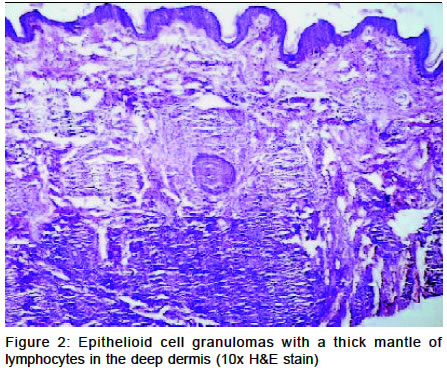
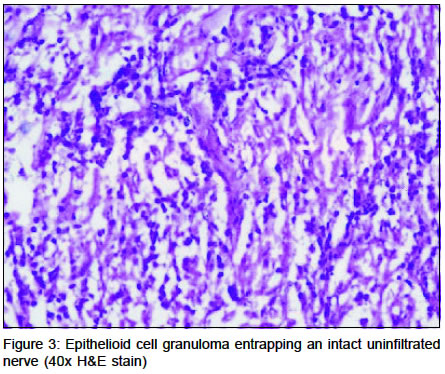
Code Number: dv03008 Abstract Acquired ichthyosis in adults may reflect internal disease, viz. internal malignancy, especially Hodgkin's lymphoma or sarcoidosis. We report a patient who developed ichthyosiform sarcoidosis over a year after completion of 6 cycles of combination chemotherapy for Hodgkin's disease. To our knowledge, the development of ichthyosiform sarcoidosis after chemotherapy for Hodgkin's disease has not been described earlier. Key Words: Hodgkin's disease, Ichthyosiform sarcoidosis Introduction Acquired ichthyosis in an adult frequently signifies internal diseases, such as sarcoidosis, malignancy (especially Hodgkin's lymphoma), leprosy, hypothyroidism, renal failure and nutritional deficiencies.1 However, ichthyosiform sarcoidosis is very rare.2 The association of sarcoidosis with Hodgkin's lymphoma has also been described.3 We describe here a patient with mixed-cellularity Hodgkin's disease, who developed ichthyosiform sarcoidosis following chemotherapy. Case report A 36-year-old man who had mixed-cellularity Hodgkin's disease (MCHD) in remission, was referred by his oncologist for dry, scaly patches over the lower legs since September 2001. He had developed pruritus and excessively dry skin in September 1999 and a progressive right cervical nodular swelling in February 2000. A lymph node biopsy had confirmed the diagnosis of MCHD, for which six cycles of COPP/ABV were given to him from March to September 2000. The patient developed subcutaneous nodules over his arms and abdomen in December 2000. A dry ichthyotic patch appeared on the posterior aspect of his right lower leg in September 2001 and a few such patches appeared over other parts of the body during the next 10 months. A few erythematous papules erupted over the left arm during January 2002 and persisted. There was no history of fever, weight loss, cough, dyspnea, chest pain, bony pains, arthralgia, hypoesthesia, paresthesia, motor deficit, nasal stuffiness, epistaxis, pedal edema, mucosal or hair involvement and eye complaints. General and systemic examination was normal, except for a solitary 1 cm, firm, mobile, non-tender right posterior cervical lymph node. Dermatological examination revealed well-defined, large, normoesthetic, ichthyotic patches over the legs (Figure 1), thighs, arms and shoulders; grouped, erythematous papules over the left arm and back, and soft to firm, mobile, non-tender, subcutaneous nodules over the arms and abdomen. There was no nerve adjacent to the patch or peripheral nerve trunk thickening. The patient also had generalized xerosis. The hair, mucosae, palms and soles were normal. A skin biopsy from an ichthyotic patch revealed well-defined epithelioid cell granulomas with a mantle of lymphocytes (Figure 2). No giant cells were seen. Nerve bundles even within the granuloma were free of infiltrate and intact (Figure 3). No acid fast bacilli were demonstrated in the biopsy or within skin clippings. The ESR was 28 mm at the end of one hour. There was polyclonal hypergammaglobulinemia, cutaneous anergy to tuberculin testing, and mild restrictive lung disease on a pulmonary function test. The hemogram, urine analysis, platelet count, blood sugar, serum creatinine, blood urea, serum calcium, liver function tests, ECG, radiograph and CT scan of the chest were normal. The serum VDRL and ELISA for HIV were non-reactive. In view of the well defined epithelioid cell granulomas without nerve involvement in the normoesthetic ichthyotic skin lesions, cutaneous anergy, hypergammaglobulinemia and restrictive lung disease, this case was diagnosed as a case of MCHD with sarcoidosis. Discussion The diagnosis of sarcoidosis is one of exclusion. In fact, it was accidental in our case as well, as prior to skin biopsy the possibility of sarcoidosis was not considered in the differential diagnosis. Later, investigations revealed a mild restrictive lung disease, cutaneous anergy and hypergammaglobulinemia. The presence of well-defined epithelioid cell granulomas deep in the dermis suggested the histopathological differential diagnosis of borderline tuberculoid leprosy, but this was ruled out by the absence of anesthesia, thickened nerves, and nerve infiltration on histopathology. There are case reports of sarcoid-like granulomas in the lymph nodes, which were interpreted as epithelioid forms of Hodgkin's disease, particularly a sub-variant of the mixed-cellularity type.4 A number of cases of Hodgkin's disease have also been described in association with sarcoidosis.3 Many cases have been described as sarcoidosis-lymphoma syndrome, where cases of proven sarcoidosis developed Hodgkin's disease many years later. Silva et al5 reported a lady, diagnosed as having sarcoidosis at the age of 13, who developed Hodgkin's disease (mixed cellularity type, stage II Bb) with local cutaneous involvement at the age of 37 and was treated with 8 cycles of MOPP/ABV with complete remission. She was still asymptomatic after 6 years of follow up. This prompted the hypothesis that sarcoidosis may predispose to a lymphoid malignancy by immune dysregulation.6 Development of sarcoidal reaction or sarcoidosis has also been reported as a reaction to Hodgkin's lymphoma and other malignancies.7 Sarcoidosis has also been reported following chemotherapy of Hodgkin's disease and other lymphoreticular malignancies, as was seen in our patient.8-11 Some authors have blamed bleomycin, which formed part of the chemotherapy received by our patient as well, as the causative agent.11 Accentuation of cutaneous sarcoid following chemotherapy of Hodgkin's lymphoma has also been reported.12 The presence of sarcoid in a case of Hodgkin's disease portends a better prognosis, due to an augmented immune reaction to the malignant cells. This was aptly demonstrated in one of the largest series, of 608 patients, of Hodgkin's disease, by Sacks et al.13 Fifty five (9%) of their patients who had sarcoid-like epithelioid granulomas (in 23 patients they involved organs spared by Hodgkin's lymphoma) had a better survival rate than the non-granulomatous group. Our patient is also relapse-free after two years of follow-up. Thus, we infer that depending on the degree of the host immune response, a localized sarcoidal reaction or generalized sarcoidosis can evolve in response to the presence of the tumor cells. The epithelioid forms of Hodgkin's lymphoma described in the literature are nothing but localized sarcoidal reactions. In the cases of sarcoidosis-lymphoma syndrome, though it has been hypothesized that the presence of sarcoidosis may cause immune dysregulation leading to lymphoreticular malignancies,6 it is not plausible as the presence of sarcoidal reaction in such cases had a better prognosis.13 Hence, the most tenable explanation for the sarcoid-lymphoma syndrome could be that a good immunological anti-tumor response of macrophages activated by T lymphocytes causes a sarcoidal reaction; thus the malignancy remains occult for many years. Similarly, cases of sarcoidosis developing after chemotherapy may be due to enhanced immune response, including to certain antigens unmasked following killing of tumor cells. References
Copyright 2003 - Indian Journal of Dermatology, Venereology & Leprology. Free full text also available from: http://www.ijdvl.com The following images related to this document are available:Photo images[dv03008f2.jpg] [dv03008f3.jpg] [dv03008f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}