 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
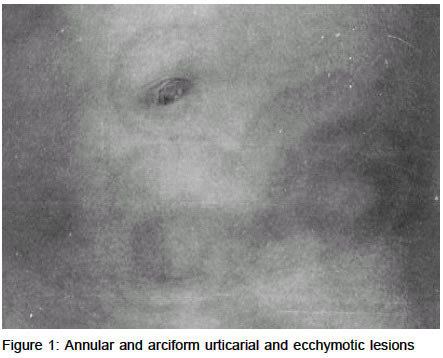
Indian Journal of Dermatology, Venereology & Leprology, Vol. 69, No. 3, May-June, 2003, pp. 223-224 Case Report Urticarial vasculitis in infancy Sukhjot Kaur, Gurvinder P. Thami Department of Dermatology and Venereology, Government Medical College and
Hospital, Sector _ 32B, Chandigarh, India.
Code Number: dv03009 Abstract Urticarial vasculitis is an uncommon manifestation of cutaneous vasculitis closely resembling chronic urticaria. It is an immune complex deposition disorder, which is not commonly observed in children. We report an 9-month-old infant with urticarial vasculitis and discuss its clinical course and differentiation from common urticaria. Key Words: Leukocytoclastic vasculitis, Hypocomplementemic vasculitis Introduction Urticarial vasculitis, an uncommon subtype of leukocytoclastic vasculitis, is characterized by recurrent episodes of urticaria lasting more than 24 hours. Constitutional symptoms such as fever, malaise and arthalgias and involvement of the internal organs, especially the kidneys and the gastrointestinal tract may also be present.1 The exact prevalence of urticarial vasculitis is not known, but it is uncommon in children.2 Case report A full-term 9-month-old male infant, born normally to non-consanguineous parents, presented with a three-day history of fever and skin rash. No history of drug intake or of similar complaints in the family was available. Examination revealed multiple, dusky erythematous to violaceous, concentric, annular and arciform urticarial wheals over the trunk, along with purpuric papules and ecchymotic plaques not blanching upon diascopy (Figure 1). General physical and systemic examination, including the eyes, mucosae and joints, was normal. Histopathology of a skin biopsy revealed leukocytoclastic vasculitis with extravasation of erythrocytes. Hemogram, serum biochemistry, urine analysis and chest X-ray were normal and anti-nuclear antibodies were negative. Treatment with a short course of oral corticosteroids and antihistaminics helped in resolution of the lesions without recurrence in 2 months' follow up. Discussion Urticarial vasculitis, also known as hypo-complementemic vasculitis or hypocomplementemic-urticaria-vasculitis syndrome is an uncommon form of leukocytoclastic vasculitis.1 It is an immune complex disorder that may occur in patients with serum sickness, SLE, Sjögrens's syndrome, infections, malignancy or as an idiopathic disorder.2 Its exact prevalence is not known and 70% of the affected individuals are females.2 It is characterized clinically by mildly itchy urticarial weals, which last for more than twenty-four hours, in contrast to common urticarial lesions that regress over 4-6 hours.3 The lesions of urticarial vasculitis possess a burning or painful quality and resolve with residual pigmentation. Often, the skin lesions have a petechial, purpuric or an echymotic element. Rarely, macular erythema, livedo reticularis, nodules and bullae may also be observed.2 Extracutaneous manifestations include constitutional features like fever, malaise, arthalgias and myalgias.2,3 Internal organ involvement, especially abdominal pain and glomerulonephritis, may occur. Histopathology reveals typical leukocytoclastic vasculitis with neutrophilic infiltration of the walls of small vessels and nuclear debris.4 Direct immunofluroscence shows immunoglobulins, complement or fibrin deposits in about one-third of patients.2 Hypocomplementemia may be present. Laboratory evaluation and therapy are similar to that described for leukocytoclastic vasculitis with corticosteroids and immunosuppressive drugs if required. Although it is a chronic and recurrent process and long-term prognosis is good, it is important to differentiate urticarial vasculitis from common urticaria as search for possible underlying etiologic factors may have prognostic implications. References
Copyright 2003 - Indian Journal of Dermatology, Venereology & Leprology. Free full text also available from: http://www.ijdvl.com The following images related to this document are available:Photo images[dv03009f1.jpg] |
| |||||||||

{kind=link}