 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Dermatology, Venereology & Leprology, Vol. 69, No. 3, May-June, 2003, pp. 232-234 Case Report Intralesional steroid induced histological changes in the skin Sukhjot Kaur, Amanjeet, Gurvinder P. Thami, Harsh Mohan Department of Dermatology & Venereology and Pathology, Government Medical
College Hospital, Chandigarh, India.
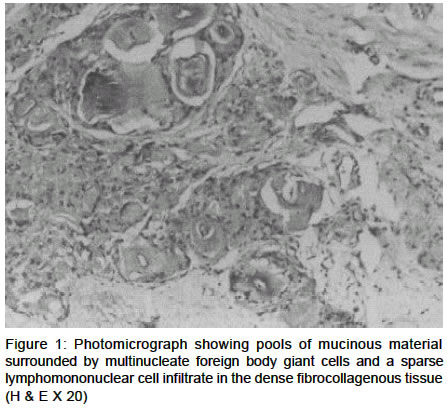
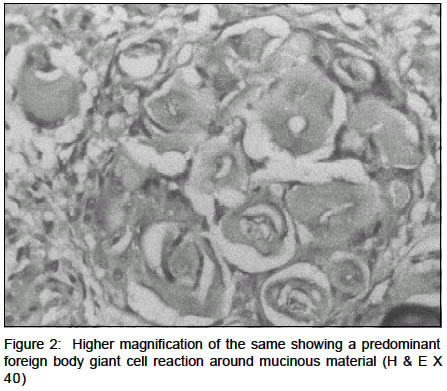
Code Number: dv03013 Abstract Intralesional steroids are commonly used in dermatology. Besides their strong anti-inflammatory effects, the long acting steroids and other preservative agents may induce interesting histopatholoical changes, which may simulate focal mucinosis or a granulomatous pathology. A variety of histopathological changes induced by Intralesional injection of steroid in a lesion of keloid are being described. Key Words: Steroid, Intralesional, Histopathology Introduction Intralesional corticosteroid injections have several applications in dermatology, the foremost being the treatment of keloids and hypertrophic scars, mostly with triamcinolone acetonide in different concentrations (10-40 mg/ml).1 The histopathology of these corticosteroid injected lesions also reveals some interesting features. The injection sites may show a deposition of acellular, lightly staining, mucinous material that may be mistaken for focal cutaneous mucinosis or a predominantly granulomatous reaction resembling rheumatoid nodule.2-4 These changes, although described in the dermatopathologic literature, are not widely recognized. We herein report the histologic changes in a patient of keloid treated with intralesional corticosteroid injections. Case Report A 42-year-old female presented with a six-month history of a 2 x 5 cm sized keloid over the anterior abdominal wall. She was initially treated with four intralesional injections of triamcinolone acetonide (40 mg/ml), which were injected at two weekly intervals, without much relief. Hence, the entire lesion was surgically removed two weeks after the last injection, to achieve resolution. The excised specimen was submitted for histo-pathological examination. The sections were stained with hematoxylin-eosin, PAS, Masson's trichrome, mucicarmine, and alcian blue at pH 1.0 and 2.5, colloidal iron and stain for fibrin. H & E stained sections revealed a normal epidermis and superficial dermis. Dense collagen bundles characteristic of a keloid were present in the deep dermis and subcutaneous tissue. Several, lightly staining, delineatnd areas of granular to amorphous, acellular mucin-like material were observed, interspersed within the collagen bundles (Figure 1). A predominantly foreign-body type giant cell reaction was noted at the periphery of these collections along with a few lymphocytes (Figure 2). There was a paucity of blood vessels in this region and histiocytes and eosinophils were absent. The material was lightly basophilic and PAS-negative. The histochemical examination excluded the fibrinous or acid mucopolysaccharide nature of the material. Discussion Local injections of corticosteroids into the skin, nasal mucosa and various soft tissue lesions results in a characteristic histologic appearance. There is deposition of a mucin-like material that is histologically observed as circumscribed, well-defined, irregularly contoured lakes of `a lightly staining material in the dermis or in the deeper tissues'.2,3 It is acellular, finely granular or amorphous and stains faintly with H & E. Although it superficially resembles mucin, it does not stain for mucin.3 The deposits are sharply demarcated in areas of dense connective tissue, while these are less well contained and less regular in looser connective tissue. The pools of mucin like material are usually surrounded by a mild cellular reaction composed of histiocytes, lymphocytes and a few foreign body giant cells.3 Occasionally, a foreign body and/or a histiocytic granulomatous response may be seen around the pools of mucin-like material, similar to a rheumatoid nodule.4 The presence of vascular proliferation with ground substance deposition as well as a paucity of blood vessels have been reported.2,3 Crystal shaped empty spaces may be observed within the mucinous material along with occasional birefringent crystals; these empty spaces are those which were probably previously occupied by corticosteroid crystals that subsequently dissolve.2 Similar histopathological changes may be observed at sites other than the skin. Balogh has reported the development of similar steroid induced changes from a ganglion, subcutaneous tissue, joints and the Achilles tendon.2 The development of necrotizing granulomas in resected polyps following corticosteroid injections has also been described by Wolff.5 The pathogenesis of these histological changes is not well understood. They probably represent a foreign body tissue reaction to either the drug itself or its solubilized vehicle, probably due to the inability of the injected material to disperse in a usual manner. The injected material persists at the injected sites, and can be recognized several weeks to months later, probably due to poor solubility of the corticosteroid crystals. The various microscopic features do not significantly vary with the type of corticosteroid, dosage, technique, different anatomic sites or the time interval between injections.2 However, others suggest that the foreign body granulomatous reaction is probably time dependent and postulate that with the passage of time the injected steroid material either diffuses or is absorbed, leaving a small amount that may act as a foreign material evoking a granulomatous response.4,5 The mucin-like deposits at the sites of corticosteroid injections have to be differentiated microscopically from focal cutaneous mucinosis, rheumatoid nodules, tophi of gout, pseudogout and myxoma. Cutaneous mucinosis is characterized by a high content of hyaluronidase-sensitive acid mucopolysaccarides and is slightly basophilic and PAS-negative. In contrast, this mucin-like deposit is distinct in that it does not show the staining qualities of an epithelial or a connective tissue mucin.7 The rheumatoid nodules have central necrobiotic material surrounded by a palisade of cells, lymphocytes, histiocytes, fibroblasts and plasma cells. Gouty tophi are similarly surrounded by a palisade-like reaction of fibroblasts, histiocytes and numerous foreign body type giant cells. The spaces occupied by urate crystals are larger, longer and needle shaped. In pseudogout, the deposits of calcium pyrophosphate dehydrate are round and smaller and do not evoke a cellular reaction. The histopathological features of corticosteroid deposits thus represent a distinct entity that should be distinguished from other similar looking conditions. Both, the clinician and the dermatopathologist should be aware of this entity to avoid misdiagnosis. References
Copyright 2003 - Indian Journal of Dermatology, Venereology & Leprology. Free full text also available from: http://www.ijdvl.com The following images related to this document are available:Photo images[dv03013f2.jpg] [dv03013f1.jpg] |
| |||||||||

{kind=link}
{kind=link}