 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
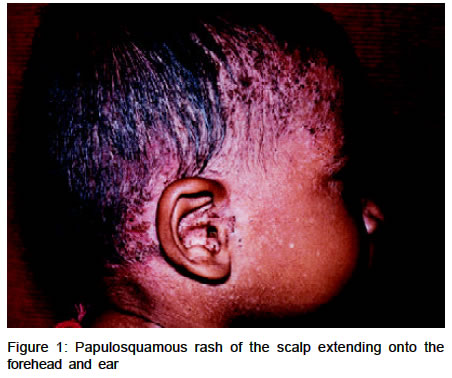
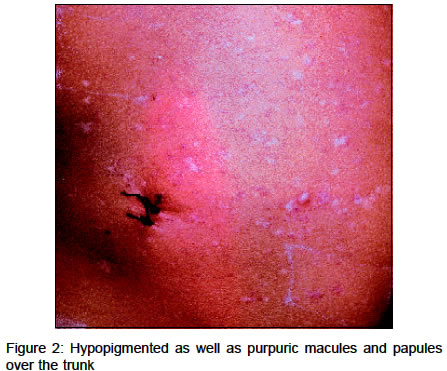
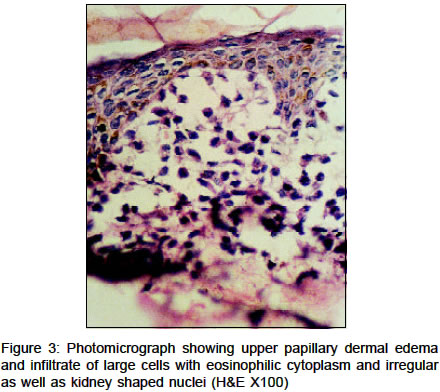
Indian Journal of Dermatology, Venereology & Leprology, Vol. 69, No. 3, May-June, 2003, pp. 241-242 Quiz S. V. Rakesh, D. M. Thappa Department of Dermatology & STD, JIPMER, Pondicherry-605006, India. E-mail: dmthappa@vsnl.net Code Number: dv03017 A 6-month-old male baby, born at full term pregnancy of non-consanguineous parents, was seen in the dermatology clinic with a 4 months' history of scaly lesions over the scalp and forehead and a purpuric rash over the trunk of three months' duration. The scalp lesions had been unresponsive to various topical antifungals applied by the mother over the past 1 month. His medical history was uneventful except for a recurrent ear discharge and intertriginous oozing dermatitis in the neck flexure over the past 3 months. His physical examination revealed diffuse erythematous greasy scaly and crusted lesions over the scalp, extending onto the forehead (Figure 1). On the trunk, multiple hypopigmented as well as minute purpuric macules and papules were seen predominantly involving the anterior abdomen (Figure 2). Apart from a cleft lip, the oral cavity demonstrated gingival hyperplasia. Systemic examination revealed gross hepatosplenomegaly. The rest of the physical examination was normal. Baseline hematological and biochemical investigations were within normal limits. Sonogram of the abdomen showed increased liver and spleen span. Histopathological examination of a biopsy taken from the purpuric papular lesion on the abdomen showed papillary dermal edema and an infiltrate of large cells with eosinophilic cytoplasm and kidney shaped nuclei. The cells infiltrated the epidermis at a few places. The epidermis was stretched and thinned out (Figure 3). His skull roentgenogram showed well-defined lytic areas with non-sclerotic borders on the cranial vault.
What is your diagnosis?
Diagnosis: Langerhans cell histiocytosis (Letterer-Siwe disease) Discussion This case illustrates the characteristic clinical, histological and radiological features of Langerhans cell histiocytosis (LCH), a reactive condition in which cells with the phenotype of Langerhans cells infiltrate in various tissues and cause damage to the tissues. These infiltrating cells are named as `LCH cells'.1, 2 Langerhans cell histiocytosis (LCH) has replaced the older term `histiocytosis-X', originally coined by Lichtenstein in 1953 to link three related clinical entities of unknown origin (Letterer- Siwe disease, Hand-Schüller-Christian disease, and eosinophilic granulomas).3 The unifying feature of these conditions is the presence of rod shaped cytoplasmic structures inside the `LCH cell' that are indistinguishable from the Birbeck granules of epidermal Langerhans cells.4 The etiology of LCH remains elusive. Viral, immunological and neoplastic pathogenic mechanisms have been considered, but none has been proved. In view of the spontaneous regression in some cases, it is believed that LCH is a non-neoplastic disease.2 Letterer-Siwe disease (LSD) is the acute disseminated multisystemic form of LCH.5 It most commonly presents in the first year of life and cutaneous involvement is an early feature. The characteristic presentation is a seborrheic dermatitis-like rash of the scalp with erythematous greasy scaling. Discrete yellow-brown scaly papules, often purpuric (representing a poor prognostic sign), may occur on the trunk. Vesicles and pustules may occur, simulating eczema, miliaria, scabies and varicella. Gingival and oral mucosal ulcerations are also commonly seen. Painful ulcerated inguinal, retroauricular, and external auditory canal nodules may occur in some patients. Temporal bone involvement may masquerade as chronic otitis media, causing a delay in the diagnosis as in our case. Marked hepatomegaly is a frequent complication and is a bad prognostic sign, particularly when accompanied by jaundice.6 Splenomegaly is less frequent. Classically, the course of LSD is rapid and fatal.2 The characteristic histological appearance of the Letterer-Siwe type of LCH is a patchy lichenoid infiltrate of large histiocytes that have a large kidney shaped, indented or bilobed nucleus and abundant homogeneous pink cytoplasm. The histiocytes frequently infiltrate the epidermis, sometimes causing a pagetoid pattern. Three kinds of histological reactions have been described in LCH, proliferative, granulomatous and xanthomatous, but only the first two are commonly seen.7 If facilities are available, marker studies for S-100 and CD1a as well as electron microscopy may be done. The management of LCH depends on the age of the patient, extent of the disease and location of the disease.2 The best option for children with only skin involvement is observation. Topical nitrogen mustard (20%) may be an effective treatment. The use of systemic glucocorticoids or anti-mitotic drugs should be considered for resistant cases. Systemic chemotherapy with prednisolone and vinca alkaloids is indicated for multi-system disease. Etoposide, cyclosporine and IFN-γ have also been reported to be beneficial in systemic disease. References
Copyright 2003 - Indian Journal of Dermatology, Venereology & Leprology. Free full text also available from: http://www.ijdvl.com The following images related to this document are available:Photo images[dv03017f2.jpg] [dv03017f1.jpg] [dv03017f3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}