 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Dermatology, Venerelogy & Leprology, Vol 69, No. 5 ,Sept-Oct, 2003, pp. 329-333 StudyPulse therapy and its modifications in pemphigus: A six year study P. Narasimha Rao, T. S. S. LakshmiDepartment of Dermatology, Osmania Medical College, Hyderabad, India.
Code Number: dv03051 Abstract Background: Dexamethasone-cyclophosphamide pulse (DCP) therapy for the pemphigus group of disorders is being widely used in India after its introduction in 1986. However, there are certain limitations to its application due to the serious side effects of cyclophosphamide. Methods: Between 1995 and 2001, we treated 41 patients of pemphigus with modified pulse therapy. These modifications included certain changes in the DCP therapy protocol and substitution of cyclophosphamide with either azathioprine or methotrexate in a few patients. Results: We observed a good response to pulse therapy in all 34 patients who took treatment regularly. Conclusions: We found the modifications to the original DCP therapy protocol to be very effective and useful. Key Words: Pemphigus, Dexamethasone-cyclophosphamide pulse, Dexamethasone-azathioprine pulse, Dexamethasone-methotrexate pulse Introduction The introduction of dexamethasone-cyclophosphamide pulse (DCP) therapy for the pemphigus group of disorders by Pasricha et al at the All India Institute of Medical Sciences (AIIMS), New Delhi, in 1986 has revolutionized the therapy for pemphigus.1 In contrast to previous reports,2 they used it to induce a permanent remission in pemphigus. At the Department of Dermatology, Osmania Medical College, Hyderabad, India, we have been using DCP therapy to treat pemphigus since 1995. Considering the necessity and acceptability of the regimen by all classes of patients of pemphigus, we have made some modifications in the methodology of DCP therapy and in the drugs used in pulse therapy. We discuss the rationale behind these changes and also our observations of the results of pulse therapy in pemphigus. Methods Forty-one patients of pemphigus enrolled for pulse therapy and followed up from 1995 to 2001 were included in this retrospective review. Exclusion criteria for pulse therapy were age below 18 years; pregnant and lactating women; and patients with uncontrolled diabetes mellitus, hypertension or severe systemic diseases where high dose steroids are contraindicated. After their informed consent was taken, they were hospitalised and relevant investigations (hemogram, routine blood biochemistry, urine exam, electrocardiogram, chest X-ray, Tzanck smear and skin biopsy in all cases and direct immunofluorescence in some patients) performed. Before every pulse, complete blood count, urine analysis, electrocardiogram, blood sugar and blood urea were measured, and after each phase, the liver function tests, chest X-ray and serum creatinine checked. Three types of pulse therapies were used: 1. Dexamethasone-cyclophosphamide pulse (DCP) of AIIMS: In phase I, dexamethasone 100 mg in 5% dextrose was given as a slow IV infusion over 2 hours for three consecutive days along with cyclophophamide 500 mg infusion on one of the days. Such pulses were repeated every 28 days till no new lesions were seen between pulses. Cyclophosphamide 50 mg/day was given orally. Phase II consisted of the DCP schedule given for a fixed duration of 6 months. In phase III, only oral cyclophosphamide 50 mg/day was given for 1 year, while in phase IV, all the drugs were withdrawn and the patient was followed-up for as long as possible. 2. Dexamethasone-azathioprine pulse (DAP): Here, cyclophosphamide was replaced by 50 mg of azathioprine daily during the first three phases. No bolus dose of azathioprine was given during the pulse. 3. Dexamethasone-methotrexate pulse (DMP): Here, cyclophosphamide was replaced by 7.5 mg of methotrexate (three doses of 2.5 mg at 12 hourly intervals) weekly given orally, during the first three phases of pulse therapy. All patients were considered for DCP therapy, but as cyclophosphamide is known to cause oligo/azoospermia and amenorrhea, for unmarried patients who had not completed their family, DAP therapy was initiated, as azathioprine has no adverse effect on the gonads. Patients on all types of pulse therapy were advised to follow contraception till all three phases of pulse therapy were completed. DMP was instituted in patients who were not completing phase I even after 12 pulses (1 year) of DCP or DAP. Other modifications in DCP were: a. All hospitalized patients were treated for intercurrent
infections and given conventional steroid therapy to control the activity of
pemphigus. The first pulse was initiated when the secondary infection was fully
controlled, existing lesions were reduced in number, and new lesions had stopped
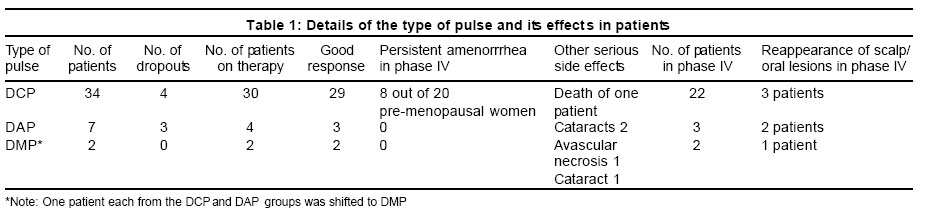
appearing. Results Of the 41 patients enrolled for pulse therapy, 13 were males and 28 females, all above 20 years of age. The majority (18) belonged to the age group of 30-40 years. Six patients had less than 10%, 18 had 10%-25%, 12 had 25%-50% and 5 had more than 50% body area involvement. On clinical and histopathological grounds, pemphigus vulgaris was diagnosed in 37 patients, pemphigus foliaceus in two patients and pemphigus erythematosus in one patient. One patient showed acantholysis on histopathology, with the clinical features being thatof subcorneal pustular dermatosis. Direct immunofluorescence (DIF) was performed in 16 patients. IgG and C3 deposits were observed in an intercellular distribution in 13 patients and along the basement membrane zone in one patient of pemphigus erythematosus. No immune deposits were observed in two patients although acantholysis was observed on histopathology. Seven of the 41 patients dropped out before completing the first 3 pulses. The results of the other 34 patients (25 female and 9 male) are shown in Table 1. Twenty-nine of the 30 patients in whom DCP was instituted showed a good response and completed phase I in an average of 8 pulses. However, one patient who had persistent skin lesions even after 12 pulses of phase I was shifted to DMP. DAP was instituted in 4 patients who were not married or had not completed their family. Out of these, 3 entered phase 4 and continue to be in remission during the last 24 months of observation. One patient who did not respond even after 18 DAPs was shifted to DMP. Both the patients who were shifted to DMP showed rapid improvement with DMP therapy and completed phase I within 4 and 6 months of starting DMP respectively. Both are in phase IV for the last 3 years and continue to be in remission. Twelve patients required oral steroid supplements ranging from 10-30 mg/day during phase I of pulse therapy. However, phase I was considered completed only when these patients did not require steroid supplementation and were free of lesions between pulses. Two patients were given 100 mg of dexamethasone pulse (DP) as an interval pulse between pulses. Scalp and oral lesions were the last ones to respond and heal in most of the patients. Local therapy in the form of intralesional steroid injections and topical potent steroids were administered in these patients in addition to pulse therapy. In our study, 54% of patients completed phase I within 6 pulses, and 75% within 9 pulses. The longest duration of phase I was 18 months in one patient (who was shifted to DMP). Overall, out of 34 patients of pemphigus on regular pulses, 27 patients entered phase IV with complete remission and effective control of their pemphigus. Seven patients are in phase III. The longest duration of follow-up of patients in phase IV is 36 months. No significant relapse or breakthrough cutaneous lesions were observed in these patients who are being followed, except in 6 patients in whom scalp lesions (4) and oral lesions (2) reappeared 6 months into phase IV. The side effects observed were mostly minor and controllable. Bacterial, fungal (candidal and dermatophyte) and viral (herpes zoster) infections were observed in 13, 5 and 2 patients respectively. Other side effects associated with high dose steroid therapy observed were steroid induced psychosis (1 patient), cataracts (3 patients), and avascular necrosis of the head of the femur (1 patient). Urinary complaints were observed in 15 patients on DCP therapy. Transient microscopic hematuria was observed in 13 patients. In 2 patients who had burning micturition and increased frequency even in phase IV, cystoscopy showed increased rugosities of the bladder. Amenorrhea was a common complaint in patients on DCP, being observed in 8 out of 20 female patients. In two patients in whom ultrasonography of the lower abdomen was performed, atrophied uterus was reported. No specific side effects of azathioprine or methotrexate were observed. The only serious complication encountered during pulse therapy was the death of a 40-year-old female patient, two days after her third DCP administration. She developed shortness of breath and died within 4 hours of shifting to the acute medical care unit due to suspected myocarditis. She had no past history of any cardiac illness. Discussion Pulse therapy for pemphigus has revolutionized the therapy for pemphigus from mere control of the disease to probable cure.4 All our patients on pulse therapy responded well to the treatment and none of them discontinued it for lack of response. In general, phase I is the most difficult phase of pulse therapy and most treatment dropouts tend to occur during this phase, as was observed in our study. We did not find the duration of the phase I to be related to the severity, extent, duration or grading of pemphigus. When we instituted pulse therapy in some patients immediately after hospitalization, we observed that they needed a higher dose of steroids between pulses. Control of secondary infection was also difficult and patient compliance was affected. Hence, we first treated their intercurrent infections and gave conventional steroid therapy to control the activity of pemphigus to the minimal level (grade I disease) which usually took 2 to 3 weeks. We found this method to be more effective in bringing about remission earlier and shortening phase I. The rationale behind the additional infusion of 500 ml of 5% dextrose on the day of intravenous cyclophosphamide administration was to wash out any retained drug in the urinary tract to prevent the urinary complications of cyclophosphamide. This was well accepted by patients, although they had to stay for a few more hours on that day. We did not encounter any serious side effect that required deferring pulse therapy in any of our patients. The transient hematuria in 13 patients on DCP was an anticipated side effect and was seen more frequently in summers, probably due to the higher concentration of cyclophosphamide in the urine. Hemorrhagic cystitis occurs in 5% to 10% of patients treated with cyclophosphamide and is believed to be caused by the metabolite acrolein.5,6 No clear relationship exists between cystitis during treatment and the long-term development of cancer. However, both squamous and transitional cell carcinomas are reported.7,8 Two of our patients who complained of urinary symptoms during phase IV had increased rugosities of the bladder wall seen on cystoscopy. These could result from chronic irritation of the bladder wall due to cyclophosphamide. Cancers may arise many years after cyclophosphamide therapy,9 and therefore continued monitoring of the lower urinary tract is indicated in patients on long-term cyclophosphamide therapy. The use of cyclophosphamide is relatively contraindicated in patients who wish to conceive children.10 Although the severity of disease may demand treatment with cyclophosphamide, the patient may be rendered infertile by the drug.11 For this reason we did not recommend DCP therapy in patients who were unmarried or had not completed their family. This is particularly important in India, where pemphigus is more common in the younger age group, compared to the west.12 The use of azathioprine instead of cyclophosphamide in such patients is logical as azathioprine does not induce gonadal dysfunction.10 Also, azathioprine has a lower risk of neoplasia compared to cyclophosphamide, and has a steroid sparing effect. In 1969, Wolff and Schriener reported the successful use of azathioprine in the treatment of pemphigus.13 Bystryn reviewed the literature and found a slightly higher rate of clinical remission with azathioprine than cyclophosphamide.14 Aberer et al reported 47% remission in a prospective long-term study of patients with pemphigus who were treated with steroids and azathioprine.15 Another study suggests a survival advantage with combined azathioprine-steroid therapy compared with either steroids or methotrexate alone.16 DAP therapy is a viable option for patients who are unmarried or have not completed their family. The use of methotrexate in the therapy of pemphigus is well known.17 However, we did not institute DMP therapy as the first choice in any of our patients. In the two patients switched to DMP because they did not complete their phase I even after 1 year, we found an excellent response, with both going into complete remission. No serious biochemical or hematological changes were observed in these patients during 5 years of study and follow-up. Methotrexate has no apparent effect on the outcome of pregnancies occurring after it is discontinued. There are no reports of abnormal children fathered by men receiving methotrexate therapy, although the sperm motility may be abnormal during treatment.18,19 Hence, apart from DAP, the DMP regimen can also be considered for patients who have not completed their family. As alternatives to the DCP regimen, the DAP and DMP regimens give more options to the patient and to the treating dermatologist. We intend to start DMP therapy directly in more patients to study its efficacy. Radiological changes of avascular necrosis of the head of the femur associated with pain in the hip were observed in one patient (who did not respond to 18 doses of DAPs and was then shifted to DMP) during phase II of pulse therapy. However, his clinical symptoms and radiological features of avascular necrosis completely resolved after 1 year of rest and supportive therapy. Prevention of osteoporosis is becoming increasingly important in patients on long-term corticosteroid therapy. Based on the schedule of supplementation in high dose glucocorticoid therapy of systemic lupus erythematosus,20 we have made supplementation with calcium 500 mg/day and intramuscular injection of Vitamin D 3 lakh units once/month as a part of the standard protocol of pulse therapy during the first two phases. The only fatal complication we encountered during the last 6 years of practice of pulse therapy was the death of a 40-year-old female patient. The exact cause of death could not be determined as an autopsy was not performed. After this episode, ECG before each monthly pulse was included as a part of the protocol. The reported serious side effects associated with intravenous administration of pulse steroid therapy include anaphylactic reactions, seizures, arrhythmias, and sudden death. Other adverse reactions include hypotension, hypertension, hyperglycemia, electrolyte shifts, and acute psychosis. Slower administration over 2 to 3 h has minimized many of the serious side effects21 and as long as vital signs are determined frequently, patients without underlying renal or cardiac disease do not need continuous cardiac monitoring.22 Pasricha et al have reported 19 deaths in 500 pemphigus patients on DCP therapy, out of which 12 were due to unrelated causes.3 Pulse therapy for pemphigus is presently being practiced in many dermatology centers all over India. Significantly, the patient compliance to this form of therapy is very good. The side effects are comparatively mild, anticipated and manageable. Importantly, no side effects of long-term steroid therapy (e.g. moon facies, weight gain, striae, hypertension, diabetes mellitus, and severe intercurrent infections) were observed in our patients. References
Copyright 2003 - Indian Journal of Dermatology, Venereology & Leprology. The following images related to this document are available:Photo images[dv03051t1.jpg] |
| |||||||||

{kind=link}