 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Dermatology, Venerelogy & Leprology, Vol 69, No. 5 ,Sept-Oct, 2003, pp. 334-337 Study Treatment of pemphigus with intravenous pulse cyclophosphamide Neeta R. Gokhale, Pradeep M. Mahajan, Rajeev R. Sule, Vasudha A. Belgaumkar, Seema M. Jain Department of Dermatology, Venereology and Leprosy, B. J. Medical
College and Sassoon General Hospitals, Pune - 411001, India.
Code Number: dv03052 Abstract Background: The complications associated with the use of systemic corticosteroid therapy have prompted a search for alternative agents. However, these agents are themselves associated with increased risk of myelosuppression or malignancy. Methods: The present study included twenty patients with recalcitrant pemphigus or steroid induced side effects who were treated with intravenous cyclophosphamide pulse therapy. Results: Out of 18 patients who completed the study, 14 showed good to excellent response. Thirteen were able to decrease their daily dose of steroid to 5-10 mg prednisolone while one could stop steroids altogether. Most patients did not experience serious side effects. Discussion: Thus intravenous pulse cyclophosphamide is a promising form of therapy in pemphigus either recalcitrant or intolerant to steroid therapy. The decreased total cumulative dose of cyclophosphamide with intravenous therapy as compared to oral therapy may reduce the incidence of secondary malignancy. Key Words: Pemphigus, Intravenous pulse, Cyclophosphamide Introduction Prior to the advent of corticosteroids, pemphigus vulgaris led to death in 90 to 100% of patients within two years either due to septicemia or electrolyte imbalance.1 After introduction of systemic corticosteroid therapy, survival has improved dramatically.2,3 However morbidity and mortality is still very high in these patients due to steroid related side effects.4 Adjuvants like azathioprine, methotrexate or cyclophosphamide are added to the treatment of pemphigus vulgaris and pemphigus foliaceus to reduce the high morbidity associated with long term oral steroids.3 However, these agents carry their own risk such as increased incidence of myelosuppression or malignancy.5 Dexamethasone pulse therapy was introduced for the treatment of pemphigus vulgaris in 1984.6,7 The current challenge is to devise a therapy with maximum efficacy and minimum side effects. With this background we evaluated the response to pulse intravenous cyclophosphamide therapy in twenty patients of pemphigus vulgaris. Methods Twenty cases of pemphigus were selected for this study. Nineteen patients were suffering from pemphigus vulgaris and one was suffering from pemphigus foliaceus. Out of the 20 patients, 13 were female and 7 were male. Two females were aged less than 20 yrs, 6 females and 5 males were between 20-50 yrs and 5 females and 2 males were between 50-70 yrs. Five females in the age group 50-70 yrs and 3 females in the group 20-50 yrs had completed their family and had undergone tubal ligation. The remaining females were counseled and advised contraception. Informed written consent was obtained from all patients. The severity of the disease was assessed as per the number of bullae/erosions according to the criteria described by Fleischi et al.8 According to these criteria, the disease is considered severe when the number of bullae/erosions exceeds 40, moderate when the number is between 20-40 and mild when the number is less than 20. We found that the number of bullae/erosions were proportional to the percentage of surface involvement. In our study, 12 patients had severe disease while the remaining 8 had disease of moderate severity. All patients had mucosal involvement.
Ten patients were already on high dose oral steroid therapy and none of them had received intravenous pulse steroid therapy. Out of these ten patients, three patients developed diabetes. Two patients developed hypertension, and one patient developed diabetes as well as hypertension. Osteoporosis was noted in one patient with hypertension while in the remaining four patients the disease was uncontrolled. Out of the ten, six patients were treated during the first episode of pemphigus while the remaining four patients were treated after relapse on high dose steroid therapy. The diagnosis was based on clinical grounds, Tzanck smear and histopathological examination. Baseline investigations like hemoglobin, white blood cell count, blood sugars, blood urea, serum electrolytes, liver function tests, X-ray chest, urine analysis and pregnancy tests (in females) were carried out.
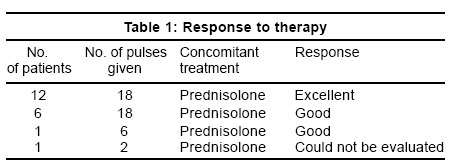
Cyclophosphamide 500 mg was dissolved in 25 ml of distilled water which was added to 500 ml of 5% dextrose and given slowly intravenously over 60 minutes.8 It was followed by 500 ml of normal saline. Vigorous oral hydration was given 24 hours before and after therapy. Similar pulses were repeated monthly for 12 months and 2 monthly for further 6 pulses. Patients were then followed for one year. Simultaneously, the dose of the steroid was tapered. Urine examination, total and differential white blood cell counts, liver function tests and platelet count were carried out every month before giving pulse cyclophosphamide. Results Out of the 20 patients, 1 patient received 6 pulses, but despite showing a good response refused further treatment. In another patient, intravenous cyclophosphamide was discontinued due to severe nausea and vomiting. Eighteen patients completed 18 pulses (Table 1).
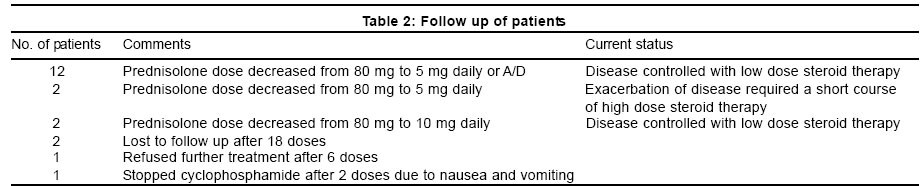
Twelve patients showed excellent response within 2-5 months with a mean duration of 3 months while six patients showed a good response within a similar period. Excellent response was considered when moderate to severe disease improved to complete clearance of disease. Good response was considered when severe disease improved to moderate and mild disease.8 In twelve patients we could taper prednisolone to 5 mg daily or on alternate days. In one patient we could stop it completely. In four patients prednisolone was tapered to 5 to 10 mg daily (Table 2). During the one year of follow up, fourteen patients remained in remission. Mild relapse (less than 20 bullae/erosions) occurred 8 and 10 months after stopping intravenous cyclophosphamide in 2 patients. In both patients, increasing the dose of prednisolone from a maintenance dose of 5 mg/day to 20 mg/day controlled the relapse. Two patients were lost to follow up after 18 pulses though both of them showed a good response. The side effects seen were nausea and vomiting in 8 patients; in 1 patient severe nausea necessitated discontinuation of pulses. She continued to take a high dose of steroids. Five women complained of amenorrhea. None of our patients developed neutropenia, sepsis or other serious side effects like hemorrhagic cystitis.
Discussion Cyclophosphamide is an alkylating agent and one of the potent immunosuppressants available today. Continuous oral cyclophosphamide has been used in dermatology for control of systemic lupus erythematosus and pemphigus.8-10 However, serious side effects like hemorrhagic cystitis, bladder carcinoma and lymphoma can occur after a cumulative dose of 85 g of cyclophosphamide.5 Intravenous cyclophosphamide has been used for lupus nephritis and for serious central nervous system involvement in lupus erythematosus.11,12 It has also been tried in fourteen patients of Wegener's granulomatosis.13 Recently, Fleischli et al used intravenous pulse cyclophosphamide therapy in nine patients of severe, recalcitrant pemphigus vulgaris.8 Six patients showed an excellent to good response, two had minimal or no response and one died. One patient relapsed. The total highest dose given was 2000 mg. The total number of pulses received by patients varied from 3 and 24.8 In our study, the response was excellent to good in all patients. Two patients developed relapse, but the disease flares were not as severe as their previous disease and could be controlled with a short course of steroid. The total highest dose given at one time was 500 mg. Eighteen of our patients completed 18 pulses. In the study by Fleischli et al,8 four patients complained of severe nausea and two had serious side effects in the form of neutropenia or sepsis. In our study, seven patients complained of nausea, which was mild, except in one patient where it necessitated stopping treatment. None of our patients developed any severe adverse reaction. Analyzing the incidence of malignancy in patients of rheumatoid arthritis treated with cyclophosphamide, Baker et al reported that the incidence depends more upon the total cumulative dose of cyclophosphamide.5 The chances of developing carcinoma bladder or hematological malignancy are high after a total dose of 85 g of cyclophosphamide. The total dose received by our patients was about10 g. As the cumulative dose with intravenous cyclophosphamide remains low, the risk of developing malignancy probably seem less with pulse therapy than with daily oral therapy of cyclophosphamide. However, long term follow-up is required. Pasricha et al7 and Kaur et al14 also reported the combination of monthly high dose dexamethasone and intravenous cyclophosphamide therapy with excellent to good response in more than 60% of patients. The disease was controlled within 2 to 3 pulses and mortality was low. In both the studies patients were required to be admitted for 4-5 days in the hospital while in our study just a single day of admission was sufficient. Thus intravenous cyclophosphamide pulse therapy can allow us to taper the steroid dose rapidly, thereby decreasing the serious side effects of steroids. Since hospitalization is required for just one day, the therapy is cost effective. It was thus possible for us to control pemphigus with
maximum efficacy and minimal side effects. These promising results
in eighteen patients
may offer us an alternative form of therapy in severe recalcitrant pemphigus
vulgaris not controlled by standard therapy or in those who cannot tolerate
steroid therapy due to diabetes, hypertension or osteoporosis. The dose
of cyclophosphamide given in our patients was uniform, viz. 500 mg
per pulse,
with 18 such pulses in 2 years. For the first time this dose of cyclophosphamide
without intravenous steroid pulse therapy was used in pemphigus. More
studies using this dose in pemphigus are warranted in future. References
Copyright 2003 - Indian Journal of Dermatology, Venereology & Leprology. The following images related to this document are available:Photo images[dv03052t1.jpg] [dv03052t2.jpg] |
| |||||||||

{kind=link}
{kind=link}