 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Dermatology, Venerelogy & Leprology, Vol 69, No. 5 ,Sept-Oct, 2003, pp. 340-342 Case Report Chilblain lupus erythematosus mimicking acrofacial vitiligo Binod K. Khaitan, Apra Sood, Rashmi Mittal, Y. Lokendra Singh, M. K. Singh*Departments of Dermatology and Venereology; and *Pathology, All India Institute
of Medical Sciences, Ansari Nagar, New Delhi - 110029, India.
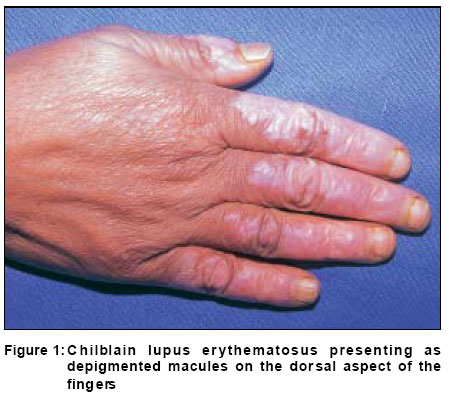
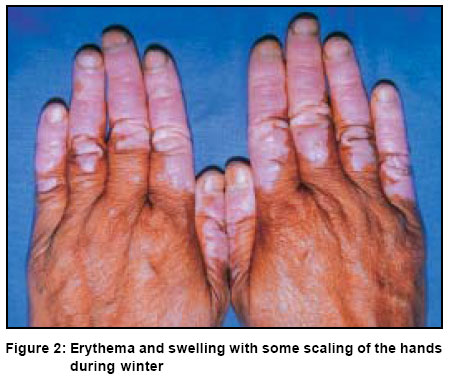
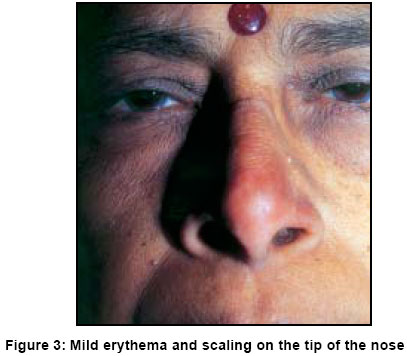
Code Number: dv03054 ABSTRACT Chilblain lupus erythematosus with depigmentation is a rare presentation of lupus erythematosus that may simulate vitiligo. A 52-year-old lady with such a manifestaiton is being reported. Key Words: Chilblain, Lupus, Vitiligo Introduction Chilblain lupus erythematosus is a chronic form of lupus erythematosus (LE) presenting mostly in women as erythematous to violaceous plaques on the acral areas and face, precipitated by cold and damp climates. Patients often have typical discoid lesions of LE in addition to chilblain-like lesions. However, when patients present with isolated chilblain lesions, the diagnosis of LE may be difficult. We report a case of chilblain LE who presented with depigmented macules on the acral areas and face resembling acrofacial vitiligo. Case Report A 52-year-old lady from western Uttar Pradesh, a region having a reasonably warm climate except for 2-3 months in a year, presented with depigmented macules on the hands, feet, nose and ears since 4 years. She complained of Raynaud's phenomenon during winters for the last 12 years. Since 8 years she had also noticed the development of mildly itchy erythematous plaques on the fingers and toes on exposure to cold. Initially these used to improve completely but since 4 years they used to heal with hypopigmentation. She was completely asymptomatic during the summers. The previous winter she had noticed similar lesions on the tip of the nose and the margins of the ear lobes. She had no history of fever, joint pain, oral ulcers, malar erythema, alopecia, photosensitivity or any other systemic complaint. She presented to us during summer with well defined, depigmented macules involving the dorsa of all the fingers (Figure 1) and toes in a symmetrical pattern involving the distal two-thirds, as well as the tip of the nose and ear lobes. The depigmented skin over the fingers had mild erythema but there was no scaling or follicular plugging in any of the lesions. The lips were not depigmented. This presentation simulated vitiligo with acral involvement. Her general physical examination and examination of the other systems was within normal limits. Investigations revealed hemoglobin 10.9 g%, total leukocyte count of 7700 (61% neutrophils, 6% eosinophils and 33% lymphocytes) and ESR of 40 mm in the first hour. Biochemical tests for hepatic and renal functions, serum proteins, urine examination and chest radiograph were normal. ANA was positive with a speckled pattern. Serum cryoglobulins were negative. A biopsy from the dorsum of the index finger revealed hyperkeratosis, irregular acanthosis, liquefaction degeneration of the basal layer and aggregation of lymphocytes around blood vessels. On direct immunoflourescence, the dermoepidermal junction revealed a linear deposit of IgM. A diagnosis of chilblain lupus erythematosus was made. She was advised protection from cold and started on topical fluocinolone acetonide 0.1% cream along with chloroquine 250 mg orally twice a day for 4 weeks followed by 250 mg once daily after baseline ophthalmological examination. Six months later, i.e. in the subsequent winter, she reported 70% improvement in the chilblain lesions as well as in Raynaud's phenomenon as compared to previous winters. At this time, the depigmented lesions were slightly raised, rather than macules, with increased erythema and scaling. Clinically, during the winter the lesions were more like chilblains with depigmentation than vitiligo (Figure 2). She also had mild erythema and scaling of the tip of the nose (Figure 3) and margins of the pinna, but there were no pigmentary changes. She was continued on the same treatment and is under follow up. Discussion Gilliam and Sontheimer classified the skin lesions of LE into six types: discoid, profound, chilblain, annular-polycyclic, papulosqamous and acute skin lesions.1 Chilblain or perniotic LE was first described by Hutchinson in 1888 as a tendency of patients to develop cold induced lesions on acral areas, which show histopathological features and immunological evidence of LE.2 The incidence of LE in patients with chilblain lesions has been reported from 7.8% to 20.5% in different series.3,4 The condition may be missed or misdiagnosed unless specifically looked for. If the climate is not cold enough the incidence may be low, which may account for the absence of such lesions in any patient in a large series on LE.5 We did not come across any report of chilblain lupus from India.6 There is a female preponderance and in some series all the patients with chilblain LE have been females.2,7 The majority of the lesions are seen during the cold weather on the toes, heels and the calves and may also be seen on the elbows, knees, ears and nose as erythematous to violaceous plaques with fissuring and hyperkeratosis. Most patients present with discoid lesions elsewhere, especially the face and head, making the condition easier to diagnose. However, isolated lesions make the diagnosis difficult unless the index of suspicion is high. Some patients of LE with erythema multiforme (Rowell's syndrome) also have chilblain-like lesions in adddition.8 Discoid lesions respond better to topical and oral steroids, whereas chilblain tend to be persistent.7 Progression to SLE has been reported in 17.6% to 20% of the cases,2,7 but is not influenced by the type and extent of the chilblains. The chilblain lesions usually evolve into DLE lesions, which may account for our patient gradually developing depigmentation at the site of the chilblains as seen in healed lesions of DLE. The pathophysiology of the lesion is still not clearly known. Vasoconstriction produced by cold along with the hyperviscosity due to immunological abnormalities like hypergamm-aglobulinemia and rheumatoid factor are thought to lead to chilblain like lesions.7 ANA is of the speckled pattern and cryoglobulins and cold agglutinin are usually negative.2,9 Therapy of chilblain LE is difficult and various drugs have been tried with variable results. A warm environment is usually the most effective preventive measure. Systemic antimalarials are thought to be effective by their anti-sludging mechanism.10 Other therapeutic modalities used have been topical andoral corticosteroids, calcium channel blockers, pentoxifylline, dapsone9 and chemicalsympathectomy.11 Our patient has so far shown a reasonably good response to a combination of chloroquine with topical fluocinolone acetonide. References
Copyright 2003 - Indian Journal of Dermatology, Venereology & Leprology. The following images related to this document are available:Photo images[dv03054f3.jpg] [dv03054f2.jpg] [dv03054f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}