 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Dermatology, Venerelogy & Leprology, Vol 69, No. 5 ,Sept-Oct, 2003, pp. 347-349 Case Report Inflammatory cutaneous metastasis as a presenting feature of bronchogenic carcinoma Arun C. Inamadar, Aparna Palit, S. B. Athanikar, V. V. Sampagavi, N. S. DeshmukhDepartments of Dermatology, Venereology & Leprology, BLDEA's SBMP Medical
College, Hospital & Research Centre, Bijapur, India.
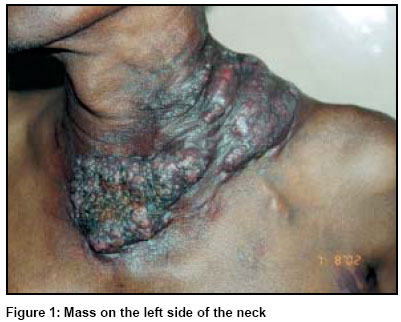
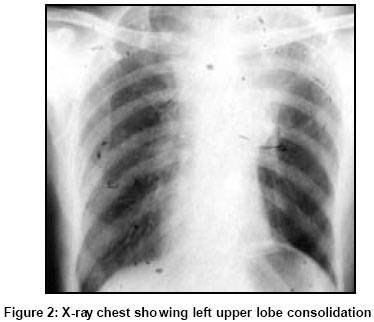
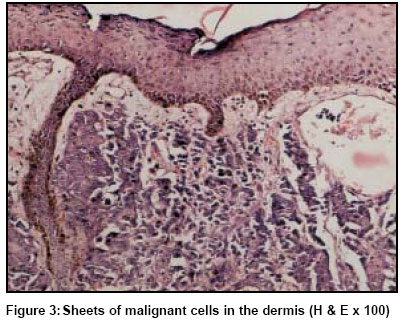
Code Number: dv03057 Abstract An elderly man with a long history of smoking presented with an excruciatingly painful mass of short duration on the left side of the neck, without any systemic complaint. Clinical and radiological examination revealed left upper lobe consolidation which was proved to be secondary to bronchogenic carcinoma. Histopathological findings from a skin biopsy from the neck mass were consistent with inflammatory cutaneous metastasis. Interestingly, this was the presenting feature of the underlying malignancy in this patient. This pattern of cutaneous metastasis has rarely been reported in association with bronchogenic carcinoma. Key Words: bronchogenic carcinoma, Inflammatory cutaneous metastasis, Carcinoma erysipelatoides Introduction The skin is a relatively uncommon site of metastasis from visceral malignancies.1 When present, it is an indicator of poor prognosis.2 Different clinical patterns are known, of which inflammatory cutaneous metastasis or carcinoma erysipelatoides is a rare variety.1 It is commonly described in association with carcinoma of the breast.1 Here, we report a patient of bronchogenic carcinoma with carcinoma erysipelatoides as a presenting feature. Case report A 60-year-old agricultural worker presented with an excruciatingly painful mass on the neck of two months' duration. It started as a small, erythematous, indurated plaque on the left side of the neck and gradually extended to the midline in front to attain the present size. There was no associated systemic complaint. He was a chronic smoker since his teens. The patient was mildly pale. His axillary lymph nodes were bilaterally palpable, and were multiple, 2-2.5 cm in size, firm to hard, discrete, mobile and tender. On examination of the respiratory system, the left infraclavicular region was flattened, with venous prominences and restricted movement of the chest wall. The trachea was shifted to the right side. The breath sounds were diminished in the left upper zone. Clinical examination of the other systems was normal. The mass on the neck (Figure 1) was about 6 inches x 4 inches in size with variable nodularity. Near the advancing edge in the midline, it showed a verrucous surface, studded with white, translucent excrescences suggestive of lymphatic stasis. It was erythematous, warm, hard in consistency and tender. Routine hematological and biochemical parameters were within normal limits. A chest X-ray (Figure 2) showed rightward shifting of the trachea, right hilar lymphadenopathy and left upper lobe consolidation. Fibreoptic bronchoscopy revealed narrowing of the lumen of the left principal bronchus with a whitish infiltrative growth with marked congestion of the mucosa. Cytological examination of the bronchial fluid revealed malignant squamous cells. Biopsy from the edge of the mass on neck showed malignant squamous cells arranged in sheets and islands in the upper dermis (Figure 3). The superficial dermal lymphatics were dilated. Biopsy from the axillary lymph nodes showed infiltration with malignant squamous cells. Ultrasonography of the abdomen was normal. A diagnosis of bronchogenic carcinoma with inflammatory skin metastasis was made and the patient was transferred to the oncology department for further management. Discussion Frequency of cutaneous metastasis from visceral malignancies is relatively low.1 However, the available data are variable. In different studies including retrospective data collected from autopsy findings, the incidence varies from 2%3 to 9%.4 Melanoma, breast and upper respiratory tract malignancies are the most frequent to metastasize to skin.3 Cervical, uterine and prostatic carcinomas are very rare causes of cutaneous metastasis.2,5,6 Skin secondaries from lung, colon and rectal carcinomas are also relatively rare.3 In the study by Lookingbill et al,2 lung malignancis ranked 15th position as a cause of cutaneous metastasis. However, in an Indian study, the commonest primary site for cutaneous metastasis among men was bronchogenic carcinoma.7 Metastasis to skin is a poor prognostic factor, as the patient usually dies within 3-6 months of diagnosis.2 Clinically common presentation of cutaneous metastasis is solitary or multiple, firm to hard , skin coloured or reddish purple nodules.1,3 Fixation to underlying tissue and ulcerations are rare.3 Several unusual morphological patterns of metastatic skin lesions are seen. These are carcinoma erysipelatoides,1 carcinoma en cuirasse,1,3 carcinoma telangiectaticum,1 Sister Mary Joseph's nodule,1 alopecia neoplastica,1 cicatricial,1,3 and bullous zosteriform metastasis.1,3,8 Carcinoma erysipelatoides or inflammatory skin metastasis was described by Hutchinson in 1893, in a patient with breast carcinoma.9 It is a rare type of cutaneous metastasis most commonly associated with breast malignancies.1,3 Rarely it occurs with malignancies of pancreas,9rectum,3 lung,9 ovary,3 parotid gland 3 and melanoma.3 To start with, there is mild erythema and slight induration of the involved area. Thereafter, there is an active spreading border, marked erythema, tenderness, increased temperature and edema, often leading to vesiculation.1 In spite of clinical resemblance to erysipelas, features of toxicity are conspicuously absent. The clinical appearance of inflammation is caused by capillary congestion. Erythema annulare centrifugum like pictures have been noted in some patients.9 Histologically, this is characterised by dilated superficial lymphatics, plugged with malignant cells and a minimal dermal inflammatory infiltrate.1 Tumour cells are not usually seen in blood vessels.2 Most frequent site of inflammatory cutaneous metastasis is local, mastectomy or thoracotomy scar or chest wall.3 Distant sites like back, forearm and neck as in the present case are sometimes involved.9 This case highlights that cutaneous metastasis may be the presenting feature of a visceral malignancy. Primaries usually presenting in this manner are lung, kidney and ovarian carcinomas.8 However, this is not a common phenomenon. As reported by Kamble et al,10 of the 471 patients of bronchogenic carcinoma they had reviewed, only 6 patients had cutaneous metastasis as the presenting feature. In the study by Lookingbill et al (1990), the incidence of cutaneous metastasis as presenting feature of lung carcinoma was only 0.6%.11 Moreover, this case represents the rare association of carcinoma erysipelatoides with bronchogenic carcinoma. References
Copyright 2003 - Indian Journal of Dermatology, Venereology & Leprology. The following images related to this document are available:Photo images[dv03057f1.jpg] [dv03057f3.jpg] [dv03057f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}