 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
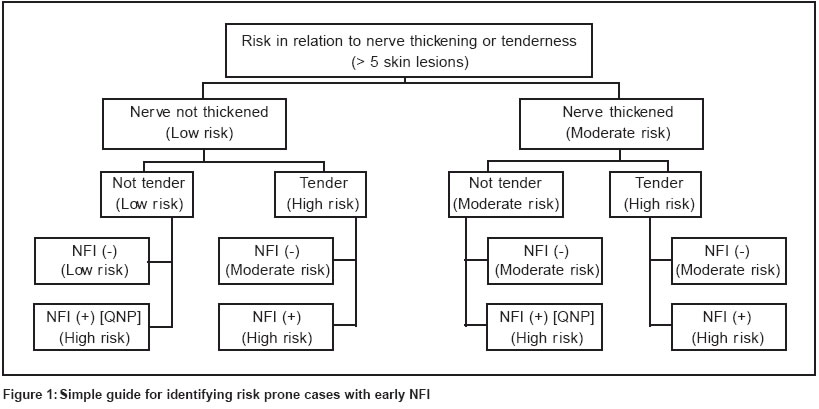
Indian Journal of Dermatology, Venereology, Leprology, Vol. 69, No. 6, Nov-Dec , 2003, pp. 369-374 Review Article Disability prevention and management in leprosy: A field experience Ganapati R, Pai VV, Kingsley S Bombay Leprosy Project, Sion Chunabhatti, Mumbai - 400 022 Code Number: dv03068 ABSTRACT Bombay Leprosy Project has conducted operational research into cost effective ways of using therapeutic management for prevention of disabilities (POD). The goal of achieving this are broadly divided as 1) prevention of impairments and disabilities [POID] and 2) prevention of worsening of disabilities [POWD]. About 33-56% of newly registered leprosy patients already have clinically detectable nerve function impairment [NFI], often no longer amenable to MDT. An analysis of 892 leprosy cases treated with WHO-MDT stresses the need to focus attention on leprosy patients having > 5 skin lesions and multiple nerve thickening. Assessment of 454 disabled leprosy patients after 4 years indicated that the compliance for the services offered was good and it helped to improve the disability status in more than 50% of patients. In terms of effectiveness of the services, it was found to be effective in preventing worsening of deformities in hands and healing of trophic ulcers in feet. The methodology adopted has also helped us to develop an operational research model about the necessity to systematize the assistance and support to be given if the services can be routed through a public health facility. Because of the large numbers of leprosy patients with disability living in this region and the limited resources available, the services have to be targeted towards those who are most in need. The major advantage of such community based program is an attempt to eliminate the social stigma in the patients' families and the education of the community.INTRODUCTION Leprosy commonly causes physical disabilities which generate social stigma. While MDT has reduced the number of people disabled by leprosy, its role in reducing the incidence of reactions and subsequent nerve damage has yet to be proved. The problems related to disabilities are not fully appreciated. There is a need to implement strategies that prevent disabilities in old cured patients and reduce their incidence in new ones.An effective leprosy control programme is required to overcome operational problems that hinder detection of new cases and identification of patients who develop nerve function impairment (NFI) after diagnosis. Prevention of disabilities (POD) can be achieved by prevention of impairments and disabilities (POID) and prevention of worsening of disabilities (POWD), but often these do not accompany the services offered towards ′medical cure′ at the grass root level. Bombay Leprosy Project (BLP), a voluntary NGO, has conducted operational research over several years to devise simple, inexpensive techniques to offer disability services at the doorstep of leprosy patients.[1],[2] These techniques have been broadly incorporated in a field based POD programme implemented in different locations.[3] We describe a broad overview of these interventions that can be practiced in the field along with the routine leprosy control programme. DEFINITION[4] Impairments′ Impairments′ are disease producing changes in the structure and functioning of certain parts of the body. They are further classified as ′primary′ (e.g. facial disfigurement, nerve and eye damage and personality disorders) and ′secondary′ (e.g. ulcers, shortening of fingers and toes, contractures and bone destruction). Disabilities Handicaps Prevention of impairments and disabilities (POID) Prevention of worsening of disabilities (POWD) EPIDEMIOLOGY Reactions or neuritis may lead to nerve damage and disabilities. Early identification of NFI and prompt treatment are crucial to prevent disabilities. About 33%-56% of newly registered leprosy patients already have clinically detectable NFI, often no longer amenable to MDT.[5] In a study in Bangladesh, 9.8% of all 786 patients with leprosy and 37.6% of the MB patients had disabilities.[6] There are no simple methods of nerve function assessment to screen risk prone cases to identify early NFI. The available methods are difficult to practice under field conditions. We analyzed the records of 892 leprosy patients treated with WHO-MDT to calculate the proportion of reaction cases in relation to the number of skin and nerve lesions at the time of registration.[7] We found that 21% of patients having >5 skin lesions had nerve involvement. It was observed that 271 patients (30%) had multiple nerve involvement and 107 patients (12%) had reactions at various stages. It was evident that the proportion of reaction showed an increase of 75% among the patients with > 5 skin lesions and multiple nerve trunk thickening at the time of registration. This analysis stresses the need to focus attention on leprosy patients having > 5 skin lesions and multiple nerve thickening. Based on this analysis, we have developed a simple guide [Figure - 1] for identifying risk prone cases with early NFI. A study in West Nepal indicates that patients with borderline leprosy having more extensive clinical disease are at a high risk for developing reversal reactions.[8] Another study found that the nerve function improved in 30%-84% (depending on the type of nerve) of 168 patients,[9] the likelihood of a ′good′ recovery being related to the severity of the nerve damage at the beginning of treatment. Of 260 newly diagnosed leprosy patients examined for NFI in Eastern Nepal, 59% had only sensory impairment (Grade 1) and 36% had one or more disabilities.[10] INTERVENTION MODELS Management of reaction or neuritis using a standard steroid regimenSimple methods to identify early nerve function impairment and treatment with a standard course of steroids [Figure - 2] make it easier for health staff to prevent deformities. Management of disabilities using simple techniques for disability care METHODS OF ASSESSMENT For POID For POWD A baseline survey of the existing POWD programme in Ulhasnagar Block, Thane District, Maharashtra[13] indicated that out of 419 deformed leprosy patients, only 25% were able to secure disability services, the compliance rate being less than 50%. After the implementation of field POWD services through leprosy workers given task oriented training, 100% service coverage was achieved in six months and the compliance rate improved from 50% to 90%. An ongoing MDT programme in a Bombay slum identified 45 disabled leprosy patients who were offered POWD services at their doorstep through CVs from the slum, under the supervision of a trained para-medical worker. A questionnaire study indicated that 82% of family members and neighbours acquired more knowledge about leprosy and actively assisted in disability care of the patients in the study area as compared to 66% in the control area where the leprosy workers offered the POWD services at the clinic. The acceptance and participation by family members was 78% in the study area and 54% in the control area.[14] In a collaborative study,[15] the nerve function of 1407 patients was monitored using standardized clinical nerve function assessment. NFI was found in 191 patients, of whom 55.9% had silent neuropathy. This study found that once NFI was clinically detectable, it was no longer at the ′early′ stage and more sensitive tests were necessary to detect real ′early′ sensory impairment in the field. This study also indicates that with well-trained field staff and proper equipment for nerve function assessment, early detection and treatment of NFI can be achieved. In Chitoor district of Andhra Pradesh,[16] where the leprosy prevalence was 15 per 10,000 population, training of the staff in POD and teaching leprosy patients self-care practices led to a remarkable improvement in skin texture and ulcers of disabled leprosy patients. In a retrospective cohort study of 786 patients in Bangladesh,[6] the incidence rate of NFI during MDT was 3.5 and 7.5 per 100 PYR in the PB group and MB group respectively. The study concluded that early detection of new cases of leprosy would prevent disabilities in more than 30% of patients and that POD activities during and after MDT would prevent disabilities in approximately 10% of patients. This study also indicates that treatment with prednisolone is effective and should be available at the field level for all patients with recent NFI. The productivity loss in India due to deformity from leprosy was assessed in a random sample of 550 leprosy patients from a rural area and an urban area in Tamil Nadu.[17] The conclusions were that elimination of deformity would raise the probability of gainful employment from 42.2% to 77.6%, and raise the overall earnings for all patients from Rs.1259 to Rs.5023 per year. Extrapolation of these findings to all of India′s estimated 645,000 leprosy patients with deformity suggested that elimination of deformity would raise productivity by Rs.130 million per year. The authors concluded that high priority should be given to the development and evaluation of programs to eliminate deformity due to leprosy. Disability care is generally considered to be expensive by experts who have considered the problem from an institutional angle, leading donors to believe that highly trained salaried staff need be employed. Considering that donor funds are scarce, any disability care strategy adopted by voluntary agencies working for leprosy control must be cost effective.[18] We believe that innovative low cost technology for offering disability care at the doorstep of the leprosy disabled is possible. The cost of offering regular disability services to one disabled leprosy patient for one year[19] at the patient′s doorstep using community volunteers is US$ 20, whereas the same offered at the clinic by leprosy workers costs US$ 240. This study also indicates the future possibility of reaching the goal of "community based rehabilitation" provided the non-leprosy handicapped in the community can be involved in a similar fashion. CONCLUSION The loss of nerve function and incapacitating deformities occurring in a small proportion of leprosy patients result in serious social and psychological handicaps that need to be overcome with help from medical personnel as a part of the management of the disease. Hence, it is important that medical and paramedical personnel know how to respond to this challenge. There are various interventional models aimed at identifying and treating leprosy patients with early nerve damage as well as established physical deformities by using simple techniques and approaches, which are practiced along with the routine leprosy control programmes. The methods of assessment of POID and POWD programmes would help to develop a feasible model to practice rehabilitation services taking into consideration the field logistics. As a result of POD activity using local health workers, a lot of awareness has been generated among the local community, which has resulted in the identification of more disabled leprosy patients than actually reported by the Government. A special questionnaire can be used to evaluate the current disability status following the services for prevention of disability. Self-care learning by leprosy patients and POD services using aids can be easily implemented by basic level health workers who have been imparted simple task-oriented training.[20] These services are effective in preventing worsening of deformities of the hands and healing of trophic foot ulcers. Because of the large numbers of disabled leprosy patients and the limited resources available, services have to be targeted towards those who are most in need. The major advantage of such a community based programme is an attempt to eliminate the social stigma in the patients′ families and the education of the community. REFERENCES
Copyright 2003 - Indian Journal of Dermatology, Venereology, Leprology The following images related to this document are available:Photo images[dv03068f1.jpg] [dv03068f2.jpg] [dv03068f3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}