 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
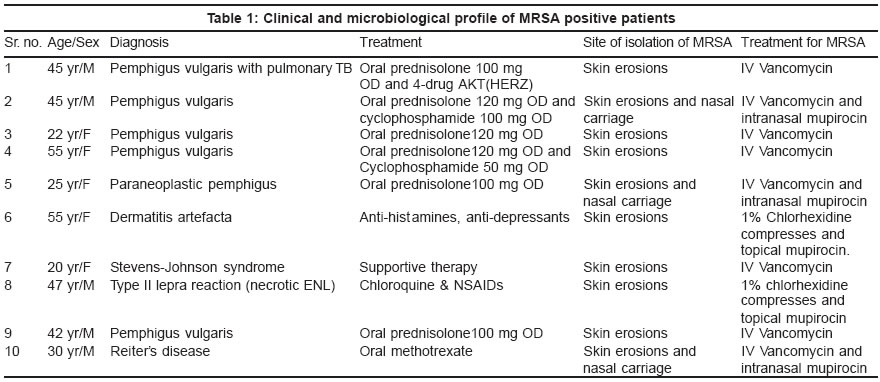
Indian Journal of Dermatology, Venereology, Leprology, Vol. 69, No. 6, Nov-Dec, 2003, pp. 377-380 Studies An outbreak of methicillin-resistant Staphylococcus aureus (MRSA) infection in dermatology indoor patients Sachdev D, Amladi S, Natraj G, Baveja S, Kharkar V, Mahajan S, Khopkar U Departments of Dermatology, Seth G. S. Medical College & K. E. M. Hospital, Mumbai Code Number: dv03070 ABSTRACT Background: Methicillin-resistant Staphylococcus aureus (MRSA) is a major nosocomial pathogen. Indiscriminate and increased use of systemic antibiotics has led to the emergence of MRSA. Infected or colonized ward patients are the main reservoir of infection. Once colonized, the risk of subsequent local and systemic infections is high, especially in the elderly, and in debilitated and immunosuppressed patients. Methods: We report an outbreak of MRSA in the dermatology ward of a tertiary care hospital and describe measures taken to control it. Results: Ten patients were found to be MRSA positive over a span of three months while screening swabs from wet lesions in indoor patients. On the basis of risk assessment, they were treated with appropriate systemic and topical therapy. One patient died while the remaining nine patients showed a good response to therapy. All the MRSA isolates were found to be sensitive to vancomycin, teicoplanin and linezolid. Conclusion: This is the first case report of MRSA infection in dermatology indoor patients in India. INTRODUCTION Methicillin, cloxacillin and flucloxacillin are penicillinase-stable beta-lactam antibiotics. Staphylococcus aureus strains which are resistant to these drugs are referred to as methicillin-resistant Staphylococcus aureus (MRSA). MRSA has been known since the 1960′s. This was soon after the introduction of methicillin for clinical use. Certain strains of MRSA were found to have the propensity to spread very quickly in hospitals. These are referred to as "epidemic" strains or EMRSA. MRSA strains are important because they have a remarkable ability to develop resistance to a variety of antibiotics including penicillins, cephalosporins, aminoglycosides, macrolides and quinolones. This poses a major threat to public health. Concern about MRSA is related to its potential for nosocomial transmission and the limited number of antibiotics available for its treatment. According to a recent Indian study, the MRSA prevalence has increased from 12% in 1992 to 80.83% in 1999.[1] Here we report an outbreak of MRSA infection in our dermatology ward. METHODS An analytical survey of the prevalence of MRSA infection among the patients of the dermatology ward in a tertiary care facility was conducted following the detection of MRSA isolates from three patients in August 2002. Screening of all the indoor patients who had erosive skin lesions and a purulent discharge revealed an additional seven MRSA isolates over the next two months. Smear, culture and antibiotic sensitivity tests were performed as per the National Committee for Clinical and Laboratory Standards Guidelines. The outbreak was reported to the Hospital Infection Control Committee and managed as per the Revised Guidelines for MRSA Control (see Discussion). All MRSA isolates were sent to the National Staphylococcal Phage Typing Centre, New Delhi. Health care workers were screened for MRSA carriage by the nasal swab technique. Swabs were also collected from environmental surfaces in the wards like beds, utensils, mattresses, dressing trolley, walls and equipment. RESULTS Out of the 63 indoor admissions from August to October 2002, MRSA isolates were detected in 10 patients, all of whom had erosive or purulent skin lesions. Thus the incidence of MRSA over these three months was 15.87%. Three of these patients showed additional evidence of nasal carriage of MRSA. In all patients, blood cultures were negative. All the MRSA strains isolated were found to be sensitive to vancomycin, teicoplanin and linezolid. The clinical and microbiological details of the study patients are summarized in [Table - 1]. Two of these patients (case nos. 6 and 8) had limited skin erosions and no constitutional symptoms. They were treated with local 2% chlorhexidine compresses and 2% mupirocin ointment. The remaining eight patients developed persistent low to moderate grade fever or progressive erosive mucocutaneous lesions with purulent discharge and were therefore administered parenteral vancomycin 15mg/kg body weight per dose twice daily for 14 days. However, one of these patients (case 1), a case of pemphigus vulgaris with pulmonary tuberculosis and malnutrition, succumbed to the disease. The remaining seven patients showed a good response to therapy. The patients were kept in isolation and barrier-nursing technique was strictly followed. Those with nasal carriage were treated with intranasal 2% mupirocin ointment thrice daily for five days. Once clinically stable, the patients were discharged on appropriate therapy for the primary skin disorder. Repeat samples of all patients were taken weekly from the previously positive sites until three consecutive results came MRSA negative. Negativity for MRSA was noted as early as 1-week post-vancomycin therapy in all patients. Screening of the staff and environmental surfaces did not reveal the presence of MRSA. Phage typing of strains from all patients revealed the strains to be non-typeable, and could not be identified as any of the common hospital related MRSA strains. The MRSA outbreak led to restriction of new indoor admissions in the ward. Strict disinfectant measures were introduced, including fumigation of the wards. DISCUSSION MRSA has recently emerged worldwide as a major nosocomial pathogen that causes significant morbidity and mortality. The major reservoirs of MRSA in institutions are infected or colonized patients. Transient hand carriage on the hands of health care workers is the predominant mode for patient-to-patient transmission. Colonization on environmental surfaces also serves as a reservoir for MRSA. The anterior nares, axillae, and perineal, perianal and inguinal regions are common sites of MRSA carriage. High carrier rates are seen in intravenous drug users and in patients with insulin-dependent diabetes mellitus. An important feature of MRSA is their propensity to spread and colonize debilitated patients. Since these strains tend to be multiple antibiotic-resistant, they pose a major difficulty in treating systemic infections. Most sensitivity studies have found MRSA isolates to be resistant to cotrimoxazole, erythromycin, gentamicin, ciprofloxacin, penicillins and cephalosporins.[1],[2],[3],[4] However, resistance to vancomycin[5] and linezolid is rare. MRSA are more pathogenic than methicillin-sensitive Staphylococcus aureus, especially in the seriously ill and immunosuppressed patients.[6] Both can cause a spectrum of illnesses ranging from minor skin infections to life-threatening complications like bacteremia and pneumonia. The risk factors for acquisition of MRSA are previous hospitalization, recent antibiotic therapy, intravascular lines, pressure sores, old age and underlying disease. Colonization with MRSA is a definite risk factor for subsequent infection.[6] Extensive colonization of the skin lesions as in burns patients increases the risk of bacteremia.[7] A delay in the initiation of effective MRSA therapy is a significant mortality risk factor. A fatal outcome has been reported in elderly patients receiving systemic corticosteroids in a dermatology day care unit.[8] The revised guidelines for MRSA control are as follows:[6]
e) Appropriate handling of laundry
3) Treatment
b) Patients who are skin carriers
c) Systemic treatment of clinical infections
Although there are several reports of MRSA in the Indian literature, these are mainly from surgical and intensive care settings. The present study is the first report of MRSA infection/colonization in dermatology indoor patients in India. The outbreak of MRSA in hospitalized patients of pemphigus, Stevens-Johnson syndrome and necrotic ENL indicates that this is a potential risk for immunocompromised dermatology patients. The additional finding of non-typeable strains in our study raises a question as to the source of the infection, whether hospital or community acquired. This report aims at creating an awareness among dermatologists about the possibility of MRSA infection in high-risk patients, especially those on steroids and immunosuppressive therapy. REFERENCES
Copyright 2003 - Indian Journal of Dermatology, Venereology, Leprology The following images related to this document are available:Photo images[dv03070t1.jpg] |
| |||||||||

{kind=link}