 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
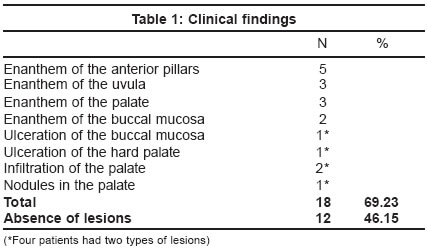
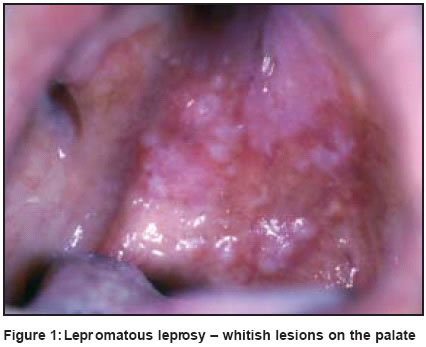
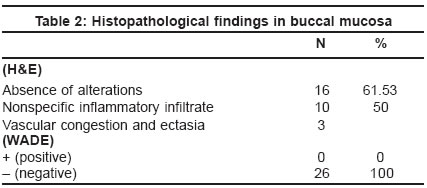
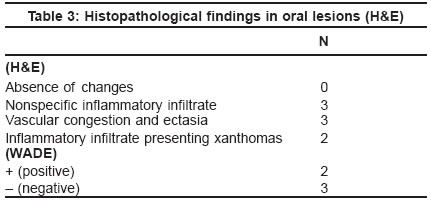
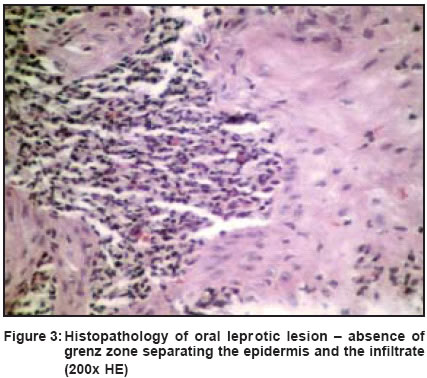
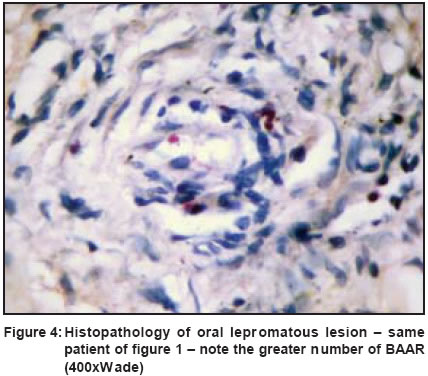
Indian Journal of Dermatology, Venereology, Leprology, Vol. 69, No. 6, Nov-Dec, 2003, pp. 381-385 Studies Oral lesions in leprosy Costa A, Nery J, Oliveira M, Cuzzi T, Silva M Department of Infectious and Parasitic Diseases, HUCFF-UFRJ and School of Medicine, Federal University of Rio de Janeiro Code Number: dv03071 ABSTRACT BACKGROUND: Leprotic oral lesions are more common in the lepromatous form of leprosy, indicate a late manifestation, and have a great epidemiological importance as a source of infection. METHODS: Patients with leprosy were examined searching for oral lesions. Biopsies of the left buccal mucosa in all patients, and of oral lesions, were performed and were stained with H&E and Wade. RESULTS: Oral lesions were found in 26 patients, 11 lepromatous leprosy, 14 borderline leprosy, and one tuberculoid leprosy. Clinically 5 patients had enanthem of the anterior pillars, 3 of the uvula and 3 of the palate. Two had palatal infiltration. Viable bacilli were found in two lepromatous patients. Biopsies of the buccal mucosa showed no change or a nonspecific inflammatory infiltrate. Oral clinical alterations were present in 69% of the patients; of these 50% showed histopathological features in an area without any lesion. DISCUSSION: Our clinical and histopathological findings corroborate earlier reports that there is a reduced incidence of oral changes, which is probably due to early treatment. The maintenance of oral infection in this area can also lead to and maintain lepra reactions, while they may also act as possible infection sources. Attention should be given to oral disease in leprosy because detection and treatment of oral lesions can prevent the spread of the disease.INTRODUCTION Leprosy is still endemic in Brazil which has the second highest number of cases in the world.[1] Oral and nasal lesions of leprosy are probably sources of spread of bacilli and transmission of the disease. These lesions are common in the lepromatous form,[2],[3],[4],[5] with the prevalence reported to range from 19% to 60% of the patients.[3],[6],[7] The presence of oral lesions is directly proportional to the duration of the disease,[8] indicating that these are a late manifestation.[2],[5],[9],[10],[11] METHODS An investigation was performed in HUCFF-UFRJ (Brazil) with the objective of studying the oral lesions in leprosy, especially in patients with the borderline and lepromatous forms. All patients with either of these clinical forms who had never taken treatment or who had received not more than one dose of MDT-MB (WHO), and who came for consultation at the Leprosy Out-Patient Clinics for one year, were screened for oral lesions. Oral lesions were biopsied and in their absence biopsies were taken of the left buccal mucosa. The biopsies were taken with a 3 mm punch, after local anesthesia, and were stained with hematoxylin-eosin (H&E) and Wade (AFB) stain. RESULTS The study included 26 patients 18 male and 8 female with leprosy whose oral lesions were evaluated and biopsied. The ages varied from 16 to 71 years. Eleven had the lepromatous form, 14 borderline, and one tuberculoid. The clinical findings are summarized in [Table - 1] [Figure - 1] and [Figure - 2]. In two lepromatous patients solid staining bacilli were found on histopathological examination. Biopsies of the buccal mucosa did not show any changes or presented a nonspecific inflammatory infiltrate, without bacilli, even in patients with lesions on the hard palate. The histopathological findings of the buccal mucosa and of the oral lesions are listed in [Table - 2] and [Table - 3] [Figure - 3] and [Figure - 4]. DISCUSSION The oral lesions in leprosy develop insidiously, are generally asymptomatic and are secondary to nasal changes.[8],[12] The most frequently affected site is the hard palate.[12],[15],[18],[20] The greater prevalence in men could be explained by the fact that women seek doctor′s advice earlier, perhaps for esthetical reasons.[5] M. leprae favors temperatures a little below the body temperature for its multiplication,[13],[14] Based on this fact, a pathophysiologic mechanism is postulated for oral involvement: a nasal lesion with obstruction of the air flow leads to oral breathing (mouth breathing), which is very common in lepromatous leprosy. This causes a decrease in the intra-oral temperature, mainly in sites near the air intake, the anterior areas, facilitating the harboring of the bacillus.[11],[13],[14] The sequence of pathological alterations would follow the same pattern described by Pinkerton in 1932 in the nasal and oral mucous membranes: congestion, infiltration, and formation of nodules, possible ulceration, atrophies and fibrosis.[3],[8],[15] Important medical and odontologic complications may follow the involvement of the oral and nasal mucous membrane and the bones of the face in leprosy.[16] In the advanced stages, there may be deformities and functional alterations, such as fibrosis and retraction of the soft palate or perforation of the hard palate, with serious disturbances in phonation, and nasal regurgitation of food.[8] Scheepers and Lemmer postulate that erythema nodosum leprosum (or reaction type II) is an important cause for destruction, perforation and deformation of the palate and uvula, alerting one to the need for more effective treatment of that condition.[17] Some authors have emphasized the epidemiological importance of oral lesions as an infection source,[5] since viable bacilli have been detected in these lesions by histopathological exam through smears and by rinsing of the oral cavity.[8] For others, the prevalence is of granulous bacilli.[9] Morphologically the lesions vary from enanthemas to ulcers, perforations and scars, passing through papules, nodules (lepromas) and superficial erosions. They can involve the following areas:
Finally, osteodental changes have also been described. Interest in these changes was raised by Møller-Christensen, a Danish archeologist, who, in 1952, when examining a cemetery of lepers of the Middle Age, verified typical bone alterations of certain parts of the face: inflammatory endonasal changes, atrophy of the forward nasal spine and of the alveolar pre-maxillary processes, with loss of the upper central and lateral incisors. He termed the facial changes resulting from these changes as facies leprosy.[21] Our findings are similar to those in the literature. Sixty nine percent of the patients presented oral clinical alterations and of those 50% showed histopathological features in an area without lesions [Table - 1] and [Table - 2]. In the two cases in which specific lesions were found, the hard palate was the site of involvement.[5],[8],[13] The areas of involvement in order of frequency, are the soft palate, the uvula and the hard palate, tongue, gum and lips.[2],[3],[4],[5],[8],[19],[22],[23],[24] Both patients with oral lesions had lepromatous leprosy, and had more numerous bacilli in the palatal lesions than in their cutaneous biopsies, which is unusual.[25] The absence of the grenz zone in oral lesions, as described by several authors,[4],[10] was observed in these two patients, a fact that could facilitate the dispersion of bacilli present in the lesions of the lepromatous patients. Histopathological changes observed in the buccal mucosa corroborate earlier reports that there are few changes in that region.[5],[8],[19] Alfieri et al studied 30 patients (15 with borderline leprosy and 15 with tuberculoid leprosy reaction) and found specific oral lesions in 8 and 5 patients respectively.[25] However, the inflammatory infiltrate in the lesions was less, with only a few bacilli. Only one case had ulceration. They concluded that in those clinical forms the oral lesions are not an important source of bacillary elimination. Pellegrino, Opromolla and Campos performed bacillary studies in leprosy patients, and found numerous acid-fast bacilli in the skin and palate, usually forming globi, and fewer bacilli in the nasal mucosa.[19] They observed a similar behavior between the bacillary regression of oral lesions and cutaneous lesions, because the oral positivity persisted in the cases in which the cutaneous lesions remained stationary or regressed slowly. Since there are many important complications of involvement of the oral and nasal mucosa and bones of the face by leprosy,[16] patients should be examined carefully and informed regarding improvement of their oral hygiene.[8] The buccal mucosa may have a normal appearance but may be involved in many cases with lepromatous leprosy, and should be examined carefully from the bacillary aspect, whenever one evaluates the incidence of leprosy lesions in the oral cavity.[2] Corroborating the idea of other authors,[4],[8],[18] it is believed that oral mucosal lesions are sources of infection in lepromatous patients who expel great numbers of bacilli when they spit, sneeze, cough or speak,[8],[18] since viable bacilli have been found in some of these lesions.[2],[11],[12],[19] Once released into the environment, the bacilli could be viable for up to nine days or even longer.[26] The lesser incidence of oral lesions observed recently compared to older reports[15] could be because the present treatment is more effective[9],[17] and is initiated earlier, and probably because of improvement in oral hygiene.[10],[27] The fact that we still see patients with oral lesions in Rio de Janeiro is highlighted here. While our study focused on oral mucosal changes in leprosy and not on dental and gingival changes, compatible with peridodontitis, nevertheless it is important to remember that the maintenance of oral infection in these structures can also lead to and maintain lepra reactions. This is an important reason to always pay careful attention to oral disease in leprosy patients under MDT. Their detection and early treatment can avoid infection of new individuals. REFERENCES
Copyright 2003 - Indian Journal of Dermatology, Venereology, Leprology The following images related to this document are available:Photo images[dv03071f4.jpg] [dv03071t3.jpg] [dv03071f1.jpg] [dv03071t1.jpg] [dv03071t2.jpg] [dv03071f3.jpg] [dv03071f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}