 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
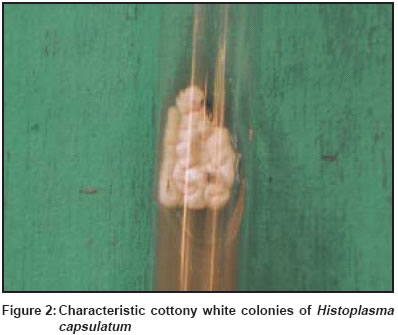
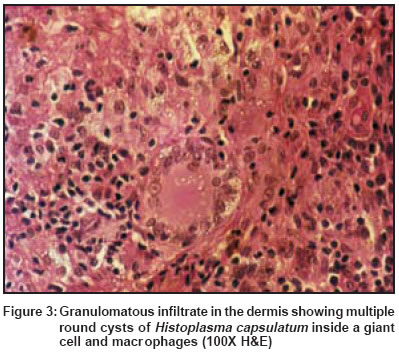
Indian Journal of Dermatology, Venereology, Leprology, Vol. 69, No. 6,Nov-Dec , 2003, pp. 405-407 Case Report Disseminated primary cutaneous histoplasmosis successfully treated with itraconazole Singhi MK, Gupta L, Kacchawa D, Gupta D Department of Skin, STD & Leprosy, Dr. S. N. Medical College, Jodhpur Code Number: dv03077 A 60-year-old immunocompetent lady with disseminated primary cutaneous histoplasmosis is reported. Histology showed a granulomatous skin infiltrate with numerous intracellular PAS positive rounded yeast cells within macrophages. Culture on Sabouraud's dextrose agar yielded a typical cottony white colony characteristic of Histoplasma capsulatum. Treatment with itraconazole showed an excellent response.INTRODUCTION Histoplasmosis, also called as Darling′s disease, is caused by a dimorphic fungus Histoplasma capsulatum.[1] The fungus has two variants viz. Histoplasma capsulatum var. capsulatum, which is found in America and the tropics, and Histoplasma capsulatum var. duboisii, which is found in Africa. Histoplasma capsulatum (the American form) mainly causes pulmonary involvement resembling tuberculosis and may pass asymptomatically to involve the reticuloendothelial system and the skin. H. duboisii mainly causes cutaneous and osseous involvement and is strictly restricted to the African continent.[1] The pulmonary and disseminated forms of histoplasmosis are very common in AIDS patients and cause great morbidity and mortality. Primary cutaneous histoplasmosis is rare. We report a case of disseminated primary cutaneous histoplasmosis caused by H. capsulatum in an immunocompetent patient on account of its rarity. CASE REPORT A 60-year-old female presented in the skin out-patient department with gradually progressive erythematous nodules and plaques distributed over the neck, chest and abdomen [Figure - 1] present since the last 2 years. She experienced mild burning and pain in the lesions. Some of them also showed spontaneous ulceration and crusting.She gave a history of residing in an area which was heavily inhabited by birds and the soil in that area contained plenty of birds′ excreta. There was no history of trauma preceding the onset of skin lesions. There was no generalized lymphadenopathy, hepatosplenomegaly or any other detectable systemic abnormality. Her general health was good. Laboratory investigations including routine haemogram, urine and stool examination, and renal and liver function tests were within normal limits. Roentgenogram of the chest and bones were normal. Mantoux test, VDRL test and ELISA for HIV were negative. Ultrasonography of the abdomen revealed a mildly enlarged liver with fatty liver change. Tissue culture for fungus on Sabouraud′s dextrose agar yielded typical cottony white buff colonies [Figure - 2] in 4 weeks. Histopathology from the lesions showed a granulomatous infiltrate involving the dermis and subcutaneous tissue mainly consisting of macrophages and scattered giant cells. Small (2-4 microns), PAS-positive, round-to-oval organisms with a clear halo were seen inside the macrophages [Figure - 3]. The dermis showed prominently dilated blood vessels with a lymphohistiocytic infiltrate. The histopathology was compatible with the diagnosis of histoplasmosis. With itraconazole 100 mg BD for 6 months, the patient showed complete clearing of lesions after 16 weeks of therapy [Figure - 4]. DISCUSSION H. capsulatum is an intracellular organism parasitizing the reticuloendothelial system and involving the spleen, liver, kidney, CNS and other organs. H. capsulatum exists as a saprophyte in nature and has been isolated from soil, particularly when contaminated with chicken feathers or droppings. Its spores are infectious to humans by the airborne route.[1] Histoplasmosis is caused by either Histoplasma capsulatum var. capsulatum, which is found in America and the tropics, and Histoplasma capsulatum var. duboisii, which is found in Africa. The African form differs from the classical American form in its clinical and pathological features. In the African form, lesions of skin and bones predominate in contrast to the American form, in which pulmonary changes dominate the clinical picture.[2] The histopathology of the African form characteristically shows a giant cell granuloma containing yeast cells 10-15 microns in diameter, whereas in the American form smaller (3-4 microns) yeast cells are embedded in histiocytes.[2] Primary cutaneous histoplasmosis is very rare. There is a report of widespread mucocutaneous histoplasmosis with papular or nodular lesions without internal involvement that resolved with amphotericin B.[3] Another report is of a patient with generalized erythroderma due to histoplasmosis who had no internal lesions.[4] Histoplasmosis is rarely reported from India, perhaps on account of its varied clinical presentation and lack of awareness amongst dermatologists. Panja and Sen first reported histoplasmosis from India in 1959.[5] Histoplasma capsulatum is considered to be endemic in certain North Indian states like West Bengal, where a study showed a prevalence of skin positivity of 9.4% to histoplasmin antigen.[6] There are a few sporadic case reports from South India as well.[7] To the best of our knowledge, no cases have been reported from the northern and western parts of India. Our patient showed widespread cutaneous lesions without any evidence of systemic involvement and immunosupression. There was no evidence of any internal organ involvement. Cutaneous nodules and plaques, which are generally seen in the African form of histoplasmosis, were associated with the histopathological features of classical histoplasmosis. Similar cases have been reported earlier.[7] Histoplasmosis usually responds to itraconazole, fluconazole or amphotericin B.[8] Our patient showed an excellent response to itraconazole 100 mg BD. The lesions started healing after 4 weeks of therapy and completely cleared in 16 weeks. Even after clearing of lesions, therapy was continued for another 8 weeks (total 24 weeks). The patient was followed up for 6 months after cessation of therapy, but there was no recurrence. The treatment was tolerated well, with no side effects. REFERENCES
Copyright 2003 - Indian Journal of Dermatology, Venereology, Leprology The following images related to this document are available:Photo images[dv03077f3.jpg] [dv03077f1.jpg] [dv03077f4.jpg] [dv03077f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}