 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
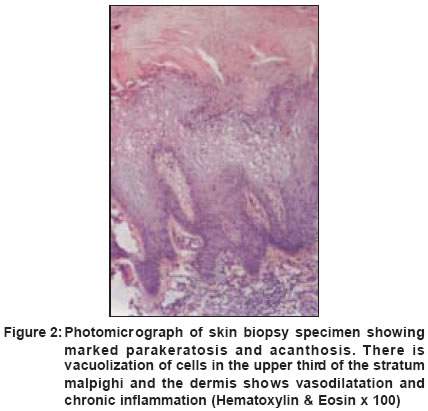
Indian Journal of Dermatology, Venereology, Leprology, Vol. 69, No. 6, Nov-Dec , 2003, pp. 425-426 Quiz Asymptomatic nodules over forearm and hand Laxmisha C, Thappa DM, Pandian S, Jayanthi S Department of Dermatology and STD, Jawaharlal Institute of Postgraduate Medical Education and Research (JIPMER), Pondicherry - 605 006 Code Number: dv03084 A 30-year-old milkmaid had asymptomatic 1.5-2.0 cms crusted nodules over her left forearm, right index [Figure - 1] and right middle finger of two and an half weeks duration. She gave a history of similar lesions occurring over the teats of her cows three weeks back. The lesions had initially started as papules, which turned vesicular in four days time and were followed by crusting a week later. There was no evidence of fever or lymphadenopathy. Histopathological examination of the skin nodule (over the finger) showed hyperkeratosis, marked parakeratosis and acanthosis. There was vacuolization of cells in the upper third of the stratum malpighi and the dermis showed vasodilatation and chronic inflammation [Figure - 2]. Higher magnification demonstrated eosinophilic inclusion bodies in the cytoplasm of vacuolated epidermal cells [Figure - 3]. WHAT IS YOUR DIAGNOSIS? Diagnosis: Milker′s nodules DISCUSSION Milker′s nodule, also known as paravaccinia or pseudocowpox, is a worldwide occupational disease of milker′s or veterinarians, caused by the paravaccinia virus.[1] It is most commonly directly transmitted from the udders of infected cows.[2] Most cases are sporadic, but small epidemics have been reported. The typical case consists of a single asymptomatic or slightly painful, one cm erythematous nodule on a finger. There are usually no more than four lesions, and they are generally confined to the hands and forearm. The incubation period is 4-7 days, but may be as long as two weeks. They usually heal spontaneously in 4-6 weeks without scar formation. Lavell and Phillips[1] have described six clinical stages, each lasting about a week. They include macular, papular, target like, nodular, granulomatous / papillomatous and regressive stage. The diagnosis in our case was based on history, clinical examination and biopsy. Histology shows the presence of vacuolated keratinocytes with intracytoplasmic inclusions (3-5 microns in size) in the first two stages, followed by multilocular vesicles with associated lymphohistiocytic dermal infiltrate and plasma cells during the third stage. Acanthosis and papillomatosis are very prominent in the 5th and 6th stages.[3] Atypical presentations without marked viral changes may potentially cause diagnostic confusion, which can be diagnosed by electron microscopy or tissue culture.[4] Other diagnostic modalities include complement fixation test and fluorescent antibody technique.[3] Although both Orf and Milker′s nodule are clinically identical, it is the source of infection: sheep and goats versus cows, which distinguishes the two.[3] Because of the clinical similarity of the two diseases, the collective term "Farmyard-pox" has been used.[4] In cow pox, the domestic cat is the source of infection and the lesions are usually painful associated with lymphadenopathy. Histologic evaluation in human cases has not revealed diagnostic cytoplasmic inclusions; but has revealed vacuolar degeneration of the epidermis.[2] Anthrax is also painless and develops an eschar by day 6.[2] The other conditions- atypical mycobacterial infection, primary inoculation tuberculosis, sporotrichosis, herpetic whitlow, etc can be differentiated based on histology and culture of the lesions. Since the disease is self limiting, only symptomatic treatment is generally indicated. One episode in humans usually induces lasting immunity.[1] REFERENCES
Copyright 2003 - Indian Journal of Dermatology, Venereology, Leprology The following images related to this document are available:Photo images[dv03084f1.jpg] [dv03084f3.gif] [dv03084f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}