 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
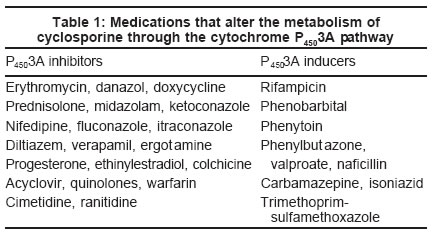
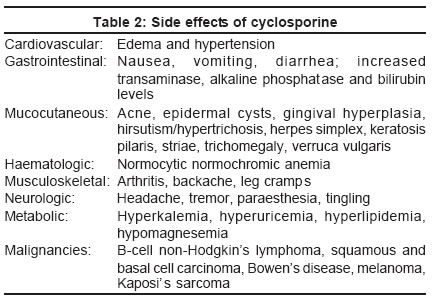
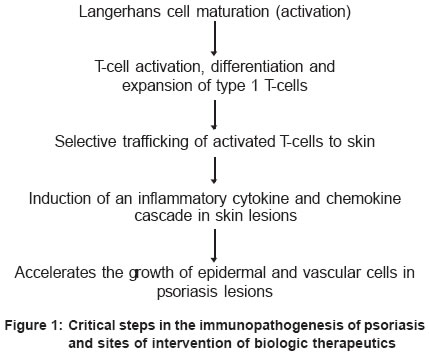
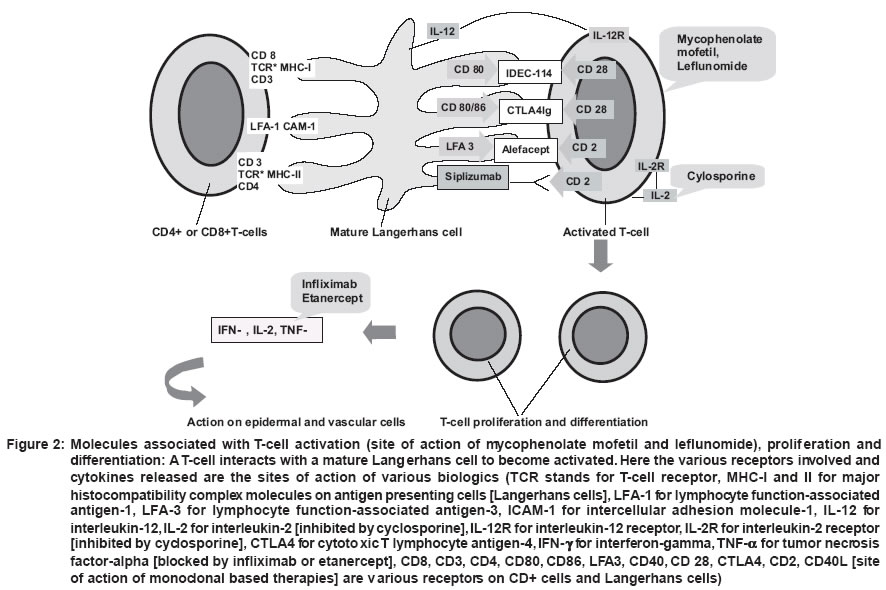
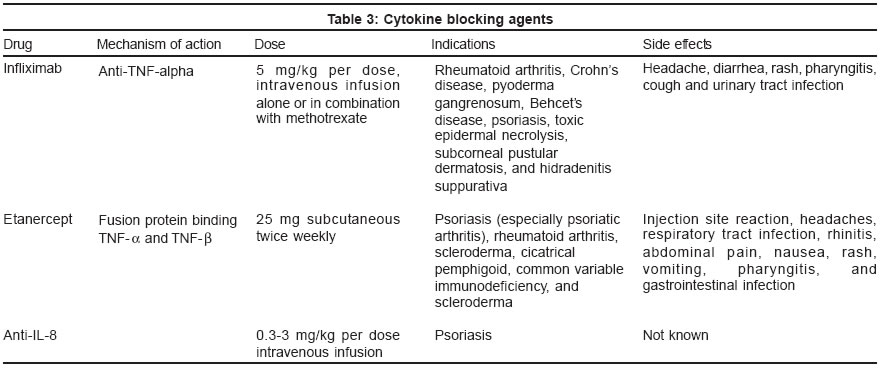
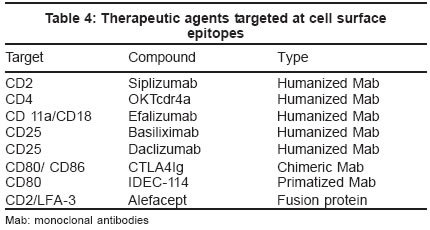
Indian Journal of Dermatology, Venereology, Leprology, Vol. 70, No. 1, January-February, 2004, pp. 1-9 Review Article Immunomodulators in the treatment of psoriasis Thappa Devinder Mohan , Laxmisha Chandrashekar Department of Dermatology and STD, Jawaharlal Institute of Postgraduate Medical Education and Research (JIPMER), Pondicherry Code Number: dv04001 ABSTRACT The efficacy of cyclosporine and related drugs in the treatment of psoriasis was the key to the development of the concept that psoriasis is an immune mediated disorder. These therapies demonstrably reduce the number of activated T-lymphocytes, which correlates with clinical remission. Monoclonal antibodies directed against key components of the inflammatory process have been studied in an attempt to produce safer, more effective and selective immunosuppressive agents. This review summarizes the information available on cyclosporine and related drugs, and cytokine therapy, including monoclonal antibodies directed against T-cell mediated inflammation. It should be realized that biologic therapies for psoriasis are very new and that efficacy and safety information from clinical trials is just becoming available.INTRODUCTION Psoriasis is a common skin disorder characterized by erythematous scaly plaques.[1] Until recently, efforts to elucidate the pathogenesis of psoriasis focused primarily on abnormal keratinocyte differentiation and proliferation. Hence, therapies were directed at decreasing keratinocyte proliferation and included topical medications (tars, anthralin, corticosteroids and salicylic acid), phototherapy (UVA and UVB), and systemic therapies (methotrexate and retinoids). Recently, it has been realized that psoriasis is an inflammatory T-cell mediated disorder. Many recent therapeutic advances are attempting to control the expression of psoriasis by suppressing T-cell mediated inflammation. Cyclosporine and related drugs, which are effective in the treatment of psoriasis, were the key to the development of the concept that psoriasis is an immune mediated disorder. These therapies demonstrably reduce the number of activated T-lymphocytes, which correlates with clinical remission. Monoclonal antibodies directed against key components of the inflammatory process have been studied in an attempt to produce safer, more effective and selective immunosuppressive agents.[1] This review summarizes the information available on cyclosporine and related drugs, and cytokine therapy including monoclonal antibodies directed against T-cell mediated inflammation. Cyclosporine Cyclosporine is a powerful immunosuppressive drug with no appreciable effect on the bone marrow.[2] It was initially discovered in 1970 at Sandoz Research Laboratories in Basel, Switzerland from two strains of fungi imperfecti, Cyclindocarpon lucidum Booth and Tolypocladium inflatum Gams. In 1978, the first human kidney transplant patients were treated with cyclosporine. A double blind study showing disease remission in psoriatic patients was reported by Ellis in 1986. Sowden demonstrated the efficacy of cyclosporine in atopic dermatitis in 1991.[2] Mechanism of action The mechanism of action of cyclosporine involves both T-cell dependent and T-cell independent effects.[3] It basically modulates immune cell function by inhibiting calcineurin-dependent dephosphorylation-activation of specific nuclear factors, thus preventing transcription of pro-inflammatory cytokines. In stimulated T cells, this drug inhibits activation by suppressing IL-2 production and IL-2R expression.[3] Recently cyclosporine has been shown to inhibit both Jun N terminal kinase (JNK) and p38 pathways. These effects are independent of calcineurin.[4]Cyclosporine also inhibits chemokine production by human mast cells, antigen presentation by Langerhans cells and neutrophil chemotaxis.[4] The main systemic side effects of cyclosporine, namely hypertension and nephrotoxicity, appear to be related to drug induced endothelin release independent of calcineurin inhibition.[5] Pharmacokinetics Cyclosporine is a lipophilic and very hydrophobic cyclic undecapeptide.[6] It is available as an oral solution, gelatin capsule and as an intravenous preparation. In general, its bioavailability after oral administration ranges from 25 to 35 per cent. Cyclosporine is metabolized into more than 30 cyclized metabolites by the liver cytochrome P4503A enzyme. It has an elimination half-life of 6-12 hours in the absence of severe hepatic disease, and biliary excretion accounts for over 90 percent of its elimination. As the primary mode of metabolism is hepatic, drugs that inhibit or induce cytochrome P4503A enzyme affect cyclosporine levels [Table - 1]. The microemulsion form is associated with faster, more extensive and predictable absorption. It is effective even in malabsorption states. Cyclosporine can also be administered intravenously as a 50 mg/ml solution made up in an ethanol-polyoxythylated castor oil mixture.[6]Although topical cyclosporine is ineffective in psoriasis, intralesional cyclosporine results in local clearing of psoriatic plaques. This appears to be related to the size of the molecule (1203 Da).[4] Dosages and monitoring In dermatological diseases, the recommended doses rarely exceed 8 mg/kg per day, with no initial loading doses. Dosage increments should not be more than 0.5-1 mg/kg per day at 2-4 week intervals.[6]According to the National Academy of Clinical Biochemistry, whole blood should be used for cyclosporine assays, with EDTA as the anticoagulant. In general, cyclosporine trough levels (whole blood concentration before next dosing) greater than 200-300 ng/ml are associated with toxicity.[6] Before putting the patient on therapy, it is mandatory to record the blood pressure (at least 2 baseline normal readings), complete blood count (CBC) with differential count, liver function tests, urinalysis (UA), and serum electrolytes including blood urea nitrogen (BUN), creatinine (Cr), and magnesium.[7] Screening during therapy involves blood pressure recording weekly for the first 6 weeks, and then monthly; CBC, electrolytes, BUN, Cr, and UA every 2 weeks for 2 months, then monthly or every 2-3 months once stable; and Cr clearance estimation every 6 months in patients on long term therapy. Indications to adjust dosage are: a) If serum Cr rises 30% above baseline, recheck in 2 weeks. If persistently elevated, decrease the dose by 1 mg/kg for one month. After 1 month at the lowered dose, if serum Cr is not within 30% of baseline, discontinue therapy until the value is within 10% of baseline. If reintroduction of cyclosporine increases serum Cr 30% over the baseline, alternative treatment should be considered; b) hypertension (mean diastolic pressure > 95 mm Hg) on two consecutive occasions requires a decreased dose of cyclosporine or introduction of antihypertensives; c) new onset hypertriglyceridemia (400-500 mg/dl) may require dose reduction; d) after 1 month, the dose can be adjusted in increments of 100 mg/d at 4-week intervals.[7] Adverse effects Nephrotoxicity and hypertension are the two most important adverse effects of cyclosporine. It can cause acute and chronic renal toxicity. Acute toxicity manifests as reversible functional changes resulting from dose dependent afferent renal arteriolar constriction, while chronic nephropathy is a progressive state of renal dysfunction due to hypertension. The risk of cyclosporine induced nephropathy can be reduced by avoiding doses greater than 5 mg/kg per day and elevation in serum creatinine 30% above baseline.[8]Cyclosporine associated hypertension usually responds to dose reduction. Patients should be asked to stop intake of all non-steroidal anti-inflammatory drugs. If medical intervention is necessary, then calcium channel blockers (nifedipine, felodipine and amlodipine) are the drugs of choice.[9] Cyclosporine does not seem to be mutagenic or teratogenic, although there is a high incidence of preterm newborns, abortions, pre-eclampsia and hypertension in mothers taking cyclosporine.[6] Apart from renal toxicity, cyclosporine has many other adverse effects, which are summarized in the [Table - 2].[7] Indications for cyclosporine The only dermatological indication for cyclosporine approved by the US Food and Drug Administration (FDA) is psoriasis.[6],[7] Given the drug′s immunomodulating effects, it has been tried in a myriad of inflammatory and non-inflammatory non-psoriatic dermatoses. A few dermatoses have been noted to have excellent response to cyclosporine: psoriasis, Behcet′s disease, epidermolysis bullosa acquisita, lichen planus and pyoderma gangrenosum.Cyclosporine is effective for the cutaneous and rheumatologic manifestations of psoriasis.[10] All forms have responded to cyclosporine. In general the more inflammatory the psoriasis, the more rapid and complete the clearing. The dose of cyclopsporine in psoriasis is 2-5 mg/kg body weight per day. For deciding the dose, the ideal body weight is taken into consideration rather than the actual body weight.[11] There are two schools of thought regarding the initial dose of cyclosporine. The Canadian and European consensus is to start the therapy at the dose of 2.5 mg/kg per day, and gradually increase it to the required amount by increasing 0.5-1 mg/kg per day every two weeks up to 4-5 mg/kg per day, whereas the American consensus is to start therapy at 4-5 mg/kg per day and after adequate response, the dose is gradually reduced by 0.5-1 mg/kg per day to the lowest effective dose or stopped. For erythrodermic and pustular psoriasis, it is recommended to start with a higher dose for prompt relief of symptoms, whereas a lower dose is needed to control plaque psoriasis. Cyclosporine is moderately effective in psoriatic arthropathy.[12] Combination therapy has been tried with methotrexate and etretinate.[6],[7] A combination with retinoids is not only efficacious, but also may protect against cutaneous malignancies. Cyclosporine produces an excellent response in most psoriatics and is an ideal agent for use as short-term monotherapy (1-2 years), in combination therapy, or as part of rotational therapy. Mycophenolate mofetil (MMF) Mycophenolate mofetil is the ester of mycophenolic acid (MPA).[15] The mofetil ester provides the advantage of increased bioavailability with improved adverse event profile. MPA is an organic acid, which was isolated as a fermentation product of Penicillium stoloniferum. It selectively inhibits inosine monophosphate dehydrogenase (IMPDH). It also induces apoptosis of activated T cells, decreases the recruitment of lymphocytes and induces immune tolerance.[13]Pharmacokinetics and drug interaction After oral administration, MMF is rapidly hydrolyzed to its active acid form, MPA.[13] After oral administration, 93% of MMF is eliminated in the urine primarily as MPA glucoronide. Because of its high affinity for plasma albumin, MPA competes with other drugs such as salicylates and furosemide that are bound to albumin; concurrent administration may lead to an accelerated elimination. As MMF and azathioprine block purine synthesis by inhibiting the same enzyme (IMPDH), MMF should not be used in combination with azathioprine.[13]Uses MMF has been found to be effective and safe in treating severe psoriasis, including erythroderma.[13] The usual dose is 1 g twice daily. Other indications for MMF are bullous autoimmune disorders, atopic dermatitis, pyoderma gangrenosum, resistant hypertrophic lichen planus and graft vs. host disease.Adverse effects Nausea, cramps, vomiting, and diarrhea are the most frequent side effects. Mild to moderate leucopenia and anemia have also been reported.[13] As it has been found to cause foetal developmental abnormalities in animal studies, contraceptive therapy is mandatory and must be continued for 6 weeks after MMF is discontinued.In summary, MMF may prove to be beneficial especially for patients who are not suited to other systemic immunotherapies because of hypertension, impaired renal function or liver disease.[13] LEFLUNOMIDE Leflunomide has demonstrated antiviral, antitumorigenic, and immunosuppressive properties.[13] Its active metabolites reversibly inhibit the mitochondrial enzyme dihydro-orotate dehydrogenase, the rate-limiting step in the de novo synthesis of pyrimidines. As a result, it inhibits autoimmune T-cell proliferation and production of autoantibodies by B-cells. Its clinical uses include rheumatoid arthritis, psoriasis vulgaris and psoriatic arthropathy, bullous autoimmune disorders, Wegener′s granulomatosis and systemic vasculitis.[13] Dosage Because of the long half-life of its active metabolites, treatment is initiated at a dose of 100 mg once daily for 3 days and continued with 10-25 mg daily.[13]Adverse effects Gastrointestinal symptoms are the most common adverse effects.[13] No significant hematopoietic toxicity, occurrence of opportunistic infections or serious mucosal toxicity was observed after its use. This drug is not recommended for female patients who are or may become pregnant.Immune-altering biologic therapy in psoriasis Recently, it has been acknowledged that psoriasis is a T-cell mediated autoimmune disease in which pro-inflammatory Th-1 cytokines play an essential role.[14] Interleukin (IL)-4 is a type 2 cytokine of decisive significance in regulating Th-1/Th-2 cytokine balance. IL-4 production is down regulated and IL-12 up regulated resulting in a type 1 response in psoriasis.[14],[15] IL-10 possesses anti-inflammatory properties and is a suppressor of cellular immunity. This action is due to inhibition of antigen presentation and production of pro-inflammatory mediators. IL-11 reduces the production of TNF-a, IL-1b and IL-12.[14] Thus, these immune pathways in cutaneous inflammation which mainly involve extracellular adhesion proteins, receptors, cytokines, and chemokines are the main targets of the new biologic therapeutic agents [Figure - 1] and [Figure - 2].[15] These protein based biologic therapeutic agents fall into 3 classes of agents: antibodies, fusion proteins, and recombinant cytokines.Initially, therapeutic antibodies were murine monoclonals that could be used for short-term administration to humans because antimurine human antibodies soon developed that blocked activity of the murine reagents.[15] Today, antibodies in therapeutic trials are mainly chimeric (fused segments of mouse and human antibodies), humanized (individual amino acids in a human backbone replaced with specific binding sequences derived from a murine monoclonal), or human sequence (generated in genetically engineered mice). Most therapeutic antibodies in trials are humanized because this technology allows for more flexibility in design of IgG isotypes and it permits reengineering of some antibody characteristics (e.g. modification of Fc receptor binding).[15] Fusion proteins are a more diverse set of molecules.[15] Often the receptor domain of a human protein is fused to constant region sequences of human IgG so that the fusion protein has binding specificity for a particular ligand or co-receptor (such as the variable region of an antibody) and so the fusion protein is soluble in plasma (such as native IgG). Alternatively, human proteins have been combined with bacterial toxins through genetic engineering.[15] The cytokines themselves and the cell surface molecules (cell surface epitopes) participating in the inflammatory process are therapeutic targets for the treatment of psoriasis.[1] Monoclonal antibodies have proven to be useful in this approach. The most common adverse effect associated with these agents is ′flu-like′ symptoms and is likely to be cytokine mediated. The term ′cytokine release phenomenon′ is often used to describe this phenomenon. This phenomenon is usually most intense early in the course of repeated administration of a monoclonal antibody, and is more intense with intravenous infusions than with subcutaneous administrations.[1] Cytokine blocking agents Cytokines are polypeptides of molecular mass less than 60 kDa. They are intercellular messengers with a pivotal role in cutaneous inflammation. The primacy of cytokines in cutaneous immune responses makes them a highly attractive target for biological response modifiers.[16] They are summarized in [Table - 3].Though targeting of cytokines is still in its infancy for the therapy of skin disease, particularly psoriasis, blocking tumor necrosis factor-alpha by infliximab or etanercept has shown particular promise, especially in the management of psoriasis.[16] Neutralizing or inhibitory antibodies to proinflammatory cytokines are the main approaches chosen by pharmaceutical companies active in the anti-cytokine arena.[16] Most of these agents have been used as a supplement in resistant and refractory cases of psoriasis. Their value as a single efficacious agent yet needs to be established. Treatment targeted to cell surface epitopes Modern biotechnology methods have enabled the generation of new types of monoclonal antibodies (Mabs) targeting cell surface epitopes [Table - 4].[17] These new agents are under investigation for the treatment of psoriasis and other dermatological disorders.[18],[19]Current data suggest that monoclonal antibodies directed against T-cell mediated inflammation are clinically effective in the treatment of psoriasis.[1] Recently, the US Food and Drug Administration (FDA) has approved alefacept for the treatment of moderate-to-severe psoriasis.[20] Alefacept, a bioengineered human fusion protein consisting of a fragment of IgG1 fused with a fragment of lymphocyte function associated antigen (LFA)-3, selectively depletes memory T cells. Lebowhl et al[21] reported the results of an international, randomized, double blind, placebo controlled, parallel group trial in 507 adults with moderate-to-severe chronic plaque psoriasis. Patients were treated with only placebo or intramuscular alefacept 10 mg or 15 mg once weekly for 12 weeks followed by 12 weeks of observation. Mean reductions in psoriasis activity and severity index (PASI) in the 15 mg alefacept, 10 mg alefacept and placebo group reached a maximum of 46%, 41%, and 25% respectively at 6 weeks after dosing. Of the patients in the 15 mg group who achieved at least 75% PASI reduction 2 weeks after the last dose, 71% maintained at least 50% improvement in PASI throughout the 12 week follow up. They concluded that intramuscular administration of alefacept is a well-tolerated and effective therapy for chronic plaque psoriasis and thus represents a convenient alternative to intravenous dosing. Krueger and Callis,[22] who reviewed the key phase II and III trials in over 1300 patients, found that about one-third of patients receiving 12 weekly intramuscular or intravenous injections of alefacept achieved a reduction in psoriasis area and severity index (PASI) scores of ³ 75% and nearly two-thirds a reduction of ³ 50%. Patients who achieved a ³ 75% reduction from baseline PASI during or after a single course maintained a ³ 50% reduction in PASI for a median duration of >7 months. Among patients who received 2 courses of alefacept, 40% and 71% of patients achieved a ³ 75% and ³ 50% reduction in PASI respectively, and the duration of effect was prolonged. Adverse events in the placebo and active treatment arms did not differ. They concluded that alefacept significantly improves psoriasis and produces durable clinical improvement with a very favorable safety profile. Thus, the strengths of alefacept are its ability to clear disease, its long lived remissions, and excellent safety profile.[20] The long lived remissions observed after cessation of treatment with alefacept, infliximab or etanercept (mainly for psoriatic arthritis) may lead one believe that these immunobiologic agents may actually alter the natural history of cutaneous manifestations of psoriasis.[22] Potential limitations in the use of these agents include the expected high costs of treatment, lack of long-term follow-up, and the selective nature of the patient populations treated thus far.[23] CURRENT STATUS OF BIOLOGIC THERAPY These biologics are administered as intravenous, intramuscular or subcutaneous injections in psoriasis where methotrexate fails.[24] Methotrexate (MTX) is used as the "gold standard" against which their efficacy is evaluated. All these biologics do produce some kind of immunosuppression, so caution may need to be exercised before they are put in use.[24] Two of the new biologic therapies have been used for other indications too.[24] Etanercept was initially approved for the treatment of rheumatoid arthritis (RA) and subsequently for the treatment of psoriatic arthritis and juvenile inflammatory arthritis. Infliximab was approved for Crohn′s disease and RA. When they first came to the US market, studies suggested that they were safe and effective. The main toxicity for etanercept was injection site reactions. The risk of serious infections, malignancy, multiple sclerosis, and autoimmune diseases was not greater than the rates that are expected in the general population. Infliximab use has been associated with the development of autoantibodies and autoimmune syndromes. With more widespread use, it has become evident that some patients treated with infliximab have reactivated dormant tuberculosis, or a systemic fungal infection, and that those treated with etanercept have developed or exacerbated pre-existing multiple sclerosis, nonmelanoma skin cancer, a drug-induced lupus erythematosus-like disease, or vasculitis.[24] Infliximab appears to be highly effective for the control of psoriasis, but the published data upon which this is based are quite small.[24] Patients with RA who were given infliximab were often concomitantly treated with an immunosuppressive agent, most often MTX, rarely azathioprine. It appears that infliximab loses its effect and is associated with more neutralizing antibodies and more infusion reactions in the absence of a concomitant immunosuppressive agent. Thus, long-term use of infliximab will not be possible without the use of a second immunosuppressive agent. This drug may find a role in the treatment of erythrodermic or pustular psoriasis.[24] Alefacept was approved for the treatment of psoriasis vulgaris in January 2003.[24] In pre-approval studies, there was seemingly little toxicity associated with its use. In a recently published study, 10% of the patients had to interrupt therapy because of CD4 counts below 250/mm[3]. Long-term use may be associated with skin cancer development in psoriasis patients who have previously received PUVA therapy.[24] Efalizumab is the fourth agent that is near market launch. It is a humanized monoclonal antibody that interrupts the interaction between CD11A and lymphocyte function-associated antigen-1.[24] It will be used as a once weekly self-administered subcutaneous injection. Experience with this drug is still limited. Lastly, adalimumab is a newly approved agent for the treatment of RA. This agent is a fully human monoclonal antibody that binds specifically to TNF-a and blocks its interaction with the p55 and p75 cell surface TNF receptors. Adalimumab also lyses surface TNF-expressing cells in vitro in the presence of complement. It is self-administered by subcutaneous injection every other week and carries a risk of reactivation of tuberculosis and serious infections, and demyelinating disease. Studies are underway to demonstrate the effectiveness of this agent for psoriasis and psoriatic arthritis.[24] Comparative data for etanercept, alefacept, and efalizumab suggested that the number of patients achieving a PASI improvement of 75% or greater was 30%, 28%, and 22.4% respectively, versus 2% to 8% for placebo, and that those achieving PASI >50% improvement were 51%, 56%, and 70% respectively.[24] In psoriasis, etanercept, alefacept, and efalizumab are at least as or more effective than MTX, but not as effective as cyclosporine, and probably not as effective as infliximab. Studies suggest that the response to efalizumab is relatively quick, while the response to etanercept and alefacept is slower.[24] Will biologics be the first line systemic therapy in psoriasis? Can biologics be used in combination therapy? It should be realized that biologic therapies for psoriasis are very new and that efficacy and safety information from clinical trials is just becoming available.[15] Presently, we cannot say which immune-targeting approach or approaches will ultimately satisfy the long-term efficacy and safety requirements for treating this chronic disease. COMBINATION, ROTATIONAL AND SEQUENTIAL APPROACHES IN THE TREATMENT OF PSORIASIS Combination, rotational, and sequential approaches are often more effective and safer than single-agent therapy.[25] Combining agents with complementary adverse effect profiles is preferable. Apparent synergistic enhancement is seen with most paired combinations of the four major therapies: acitretin, phototherapy (ultraviolet B/psoralen plus ultraviolet A), cyclosporine, and methotrexate. Of these, only cyclosporine in combination with psoralen plus ultraviolet A is contraindicated because of an increased cancer risk. Combinations of each of those major therapies with topical agents (retinoids, steroids, vitamin D derivatives, and others) have been used with varying efficacy and safety. The immunomodulators hydroxyurea and thioguanine have also shown some success in combination therapy. The new biologic agents with their novel modes of action and adverse effect profiles may prove to be important adjuncts in combination, rotational and sequential approaches.[25]REFERENCES
Copyright 2004 - Indian Journal of Dermatology, Venereology, Leprology The following images related to this document are available:Photo images[dv04001f1.jpg] [dv04001t2.jpg] [dv04001t1.jpg] [dv04001t4.jpg] [dv04001t3.jpg] [dv04001f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}