 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
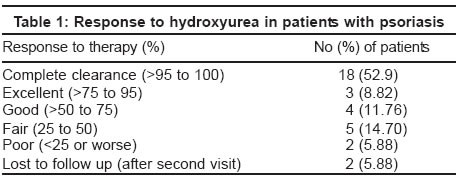
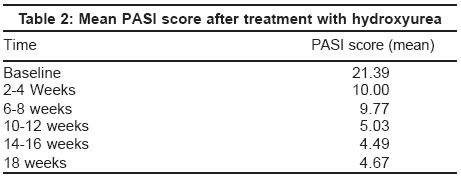
Indian Journal of Dermatology, Venereology, Leprology, Vol. 70, No. 1, January-February, 2004, pp. 13-17 Studies Hydroxyurea as an alternative therapy for psoriasis Sharma Vinod Kumar , Dutta Bornali , Ramam M Department of Dermatology and Venereology, All India Institute of Medical Sciences, New Delhi Code Number: dv04003 ABSTRACT Background: Methotrexate is the drug of choice in extensive psoriasis in developing countries. In patients who can not take methotrexate either due to intolerance or concomitant liver disease, there is an urgent need for an alternative affordable and accessible drug. Aims: To evaluate the therapeutic efficacy and safety of hydroxyurea as an alternative in the management of patients with extensive psoriasis. Methods: A prospective study was carried out over 16 months on 34 patients with chronic plaque psoriasis (>20% body surface area involvement), erythrodermic or generalized pustular psoriasis who were partially responsive or non-responsive to the conventional topical and systemic modalities of therapy. Besides doing a baseline hemogram, liver and renal function tests, and urine analysis, these tests were frequently repeated during the course of therapy. Hydroxyurea was started at 1 g daily and increased to 1.5 g, if required. The therapeutic response was evaluated by a global assessment made by the patient and physician and regular PASI scoring. Results: Good to excellent response was observed in 25 (73.5%) patients, less than 50% response in 7 (20.6%) patients, while 2 (5.9%) patients were lost to follow up. The mean PASI score was reduced by 76% at 10-12 weeks. Therapy was discontinued in 3 patients due to leukopenia that recovered on discontinuation of hydroxyurea. Patients were followed up to 1 year and relapse was observed in 5 patients. The duration of remission varied from 6 months to 1 year. Conclusion: Hydroxyurea is an effective and reasonably safe second line agent for psoriasis.INTRODUCTION Psoriasis is a chronic skin disease that seriously affects the quality of life. Treatment is aimed at making patients almost lesion free, thereby making them presentable and comfortable. In many developing countries, psoriasis is managed with topical modalities, and when systemic treatment is indicated, methotrexate is the drug of choice as cyclosporine is too expensive, acitretin is not freely available and PUVA chambers are available only in a few cities. There is an urgent need for an alternative to methotrexate in those where methotrexate is contraindicated or not tolerated. We evaluated hydroxyurea for the treatment of extensive psoriasis.[1],[2],[3] METHODS All consecutive adult patients with psoriasis attending the dermatology outpatient department of the first author in a tertiary hospital were considered for the study in the year 2000-2001. Hydroxyurea was considered for the treatment of patients with the following parameters: Pregnant and lactating women and children were excluded from the study. Pregnancy was excluded by a history of amenorrhea, and a pregnancy test was done if necessary. Men and women in the reproductive age group were advised contraception during the therapy period. The severity of disease was assessed in the first visit in all patients by calculating PASI (Psoriasis Area and Severity Index). Prior to starting therapy, laboratory investigations like hemoglobin percentage, total leukocyte count (TLC), platelet count, renal function tests, liver function tests and routine examination of urine were performed. The starting dose for all patients was hydroxyurea 500 mg twice daily. After a week, the baseline investigations, particularly the hemogram, were repeated and therapy was continued if they were within normal limits. Patients were monitored every 2 weeks for blood counts and clinically assessed at monthly intervals. Hydroxyurea was stopped if the TLC was <4000 and the platelet count was <100,000. Later, when the TLC and platelet counts returned to normal, hydroxyurea was restarted at lower doses if patients had a good response. The clinical course was evaluated by a global assessment made by the patient and the physician and the PASI score at 1 week, 3 weeks and subsequently at 4-weekly intervals. If after 2 weeks, the reduction in the PASI score was <25% and global assessment showed <25% improvement, the dose of hydroxyurea was increased to 1 g/1.5 g on alternate days and later 1.5 g daily, keeping a close watch on the hematological parameters. The treatment was continued till complete or near complete (>95%) clearance and then tapered over a period of 4-8 weeks. Residual or resistant lesions were managed with topical coal tar, dithranol and emollients. Pigmentation of the proximal aspect of the nails and alteration of counts were taken as indirect parameters for assessing compliance. Patients were followed at 4-6 weekly intervals after clearance to assess the duration of remission. The response was graded as complete clearance (more than 95% lesions cleared), excellent (>75-95% clearance), good (>50-75% clearance), fair (>25-50% clearance) or poor (less than 25% clearance or the disease worsened). If 25-50% improvement was not achieved by 8 weeks, the response was considered inadequate and the patient was offered the option of alternative therapy. RESULTS Forty patients (32 men and 8 women) with psoriasis were considered eligible for hydroxyurea therapy. Three did not return after investigations and another three were not considered fit for treatment with hydroxyurea because of concurrent medical problems (carcinoma cervix, hepatitis B and extensive tinea corporis). In the remaining 34 patients (29 men and 5 women), the average duration of illness was 6.5 years and the mean age at presentation was 37.3 years. The clinical types were chronic plaque psoriasis in 26 patients, erythrodermic psoriasis in 4, pustular psoriasis in 3 and sebopsoriasis in 1 patient. All the patients had received topical treatment and a majority had taken systemic therapy. Three patients had been treated earlier with PUVA-SOL, 10 with systemic steroids and 11 with methotrexate with partial or no response, intolerance or aggravation. Twenty-five (73.52%) out of the 34 patients had a good to excellent response and 7 (20.59%) patients had less than 50% response [Table - 1]. Two patients were lost to follow up after treatment with hydroxyurea. Responders started showing improvement by 2 weeks of starting therapy. Patients who cleared completely with hydroxyurea showed 50-75% improvement by 4 weeks and became lesion free by 8-12 weeks. Patients with good to excellent response also behaved similarly, but a few resistant lesions persisted on lower abdomen, buttocks, scalp, shin, elbows, palms and soles, and were managed with topical therapy alone. Six patients received a dose up to 1.5 g; two cleared by 8 to 10 weeks, two developed leukopenia without clinical improvement, one remained unchanged and one worsened. A 76% reduction in mean PASI score was seen at 10-12 weeks with almost a plateau thereafter; the mean PASI score reduction at 14 to 16 weeks was 79% [Table - 2]. Patients who had shown aggravation (n=1) or inadequate response (n=2) with topical and systemic puva-SOL responded by complete clearance by 10 to 12 weeks (n=1) with hydroxyurea. Systemic steroids had caused aggravation in 4 patients; 2 cleared by 12-16 weeks with hydroxyurea, while 2 showed 90-95% improvement by 6 weeks. Patients with a poor response to systemic steroids responded by 95% improvement by 8-12 weeks (n=4, 1 required a higher dose), 75-95% improvement by 8-10 weeks (n=1), and 50-75% improvement by 10 weeks (n=1). Hydroxyurea brought about complete clearance in 5 patients who had intolerance or concomitant liver disease due to methotrexate; 1 relapsed on stopping hydroxyurea. Out of the 6 patients who had partial success with methotrexate, 2 responded by complete clearance by 7-8 weeks, and 2 had 80% improvement by 8 weeks, whereas the drug was stopped due to leukopenia in 1 patient, and 1 stopped it on his own. After stopping therapy, patients were followed up to 1 year. Relapse was observed in 5 patients who had stopped treatment on their own due to complete clearance of the psoriasis, and in 1 who had improvement but had stopped treatment on his own due to a fall in blood counts. The duration of remission ranged from 6 months to 1 year. Relapses were managed with topical therapy, methotrexate, and PUVA-SOL in one patient each and hydroxyurea in 2 patients. Leukopenia was observed in 5 patients at 4-6 weeks; treatment was temporarily discontinued in 2 patients with 75-95% clinical improvement and restarted with hydroxyurea 500 mg twice daily, while 3 patients were discontinued from therapy because of falling counts and no clinical improvement. Three patients had thrombocytopenia (in one patient leukopenia and thrombocytopenia co-existed), which was managed by reducing the dose of hydroxyurea. Other side effects were skin infections (8 patients; 5 had a bacterial, 2 had a dermatophytic, and 1 had a viral infection), dry skin (3 patients), diffuse reversible alopecia (2 patients), and anemia (1 patient). Pruritus, joint pain, loose motion, weight gain were encountered in one patient each. Post-inflammatory lesional and nail hyperpigmentation were seen in all patients. DISCUSSION Hydroxyurea is an antimetabolite agent. Though its exact mechanism of action is unknown, it probably inhibits deoxyribonucleic acid (DNA) synthesis by interfering with the catalytic activity of the enzyme ribonucleoside diphosphatase reductase. Its action is specific for the S-phase of the cell cycle.[4] Hydroxyurea was first reported as an effective anticancer agent in 1960. Yarbro was the first to report on its efficacy in clearing refractory psoriasis in 1969.[5] In different studies, it has been found to result in improvement in 50% cases of refractory psoriasis in a dose of 1 g twice daily;[6] in a good to excellent response in 63% of patients (including erythrodermic and pustular psoriasis);[7] in complete to near complete clearance in 60%, and partial clearance in 20% of patients at 0.5-1.5 g daily;[8] in a substantial but slightly slow response in 66.7% of patients;[9] and in an adequate response in 75% of patients, with more than 50% showing more than 70% reduction in the PASI score[2]. It is effective in psoriatic erythroderma and guttate psoriasis,[7] but shows a variable response in pustular psoriasis.[10],[11],[12] In our study, the response in patients with plaque psoriasis was at par with most previous studies. Of the 4 patients with psoriatic erythroderma, 2 cleared completely by 12 weeks, 1 discontinued treatment due to leukopenia and 1 was lost to follow up. In contrast to some previous studies,[10],[11] 2 out of 3 of our patients with generalized pustular psoriasis showed a good to excellent response. It has been thought that patients who respond poorly to methotrexate or PUVA are refractory to hydroxyurea too, but this notion has been refuted for both systemically and topically recalcitrant disease.[8],[13] All our patients who had not responded to topical or systemic therapy (steroids, PUVA-SOL, methotrexate intolerance) had a good to excellent response to hydroxyurea. It is difficult to comment on the effect of hydroxyurea on the natural course of psoriasis. Some authors have observed a longer remission while others have not.[8],[14] Five of our patients relapsed. The period of remission was longer when the drug was gradually tapered and stopped. Further double blind studies are needed to confirm this observation. The main concern regarding hydroxyurea is myelosuppression, which manifests as anemia, thrombocytopenia or leukopenia.[5],[7],[8] As with most previous studies, our patients had mostly mild and unremarkable side effects. During our 16-month study period we did not observe unusual complications like dermatomyositis, leg ulcers, dermopathy and lupus erythematosus.[15],[16],[17] We had to stop therapy in 3 patients who had developed leucopenia (TLC < 4000). A gradual increase in the dose from 1 g daily to 1.5/1 g on alternate days and, if needed, to 1.5 g daily is safer and may prevent leukopenia in some cases. Hydroxyurea can also be safely prescribed to patients with common systemic disorders such as hyperlipidemia, mild renal insufficiency and cardiopulmonary disease, in whom other systemic medications like acitretin or cyclosporine may not be advisable. A cost comparison of systemic therapies for psoriasis shows that PUVA-SOL is the cheapest followed in ascending order by methotrexate, hydroxyurea, acitretin and cyclosporin. In conclusion, hydroxyurea is a good second line systemic agent for psoriasis. It is relatively inexpensive and has few contraindications. It is a relatively less toxic drug than imagined, not only for plaque psoriasis, but also for erythrodermic and pustular psoriasis. The commonly dreaded side effect of this drug, myelosuppression, is relatively uncommon at the doses required to treat psoriasis (1-1.5 g) and is reversible. REFERENCES
Copyright 2004 - Indian Journal of Dermatology, Venereology, Leprology The following images related to this document are available:Photo images[dv04003t2.jpg] [dv04003t1.jpg] |
| |||||||||

{kind=link}
{kind=link}