 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
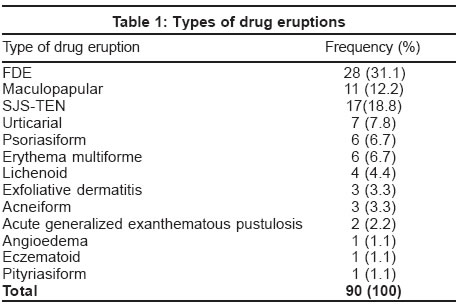
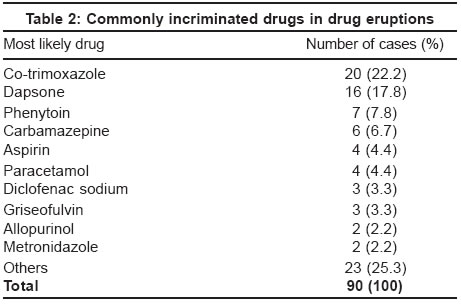
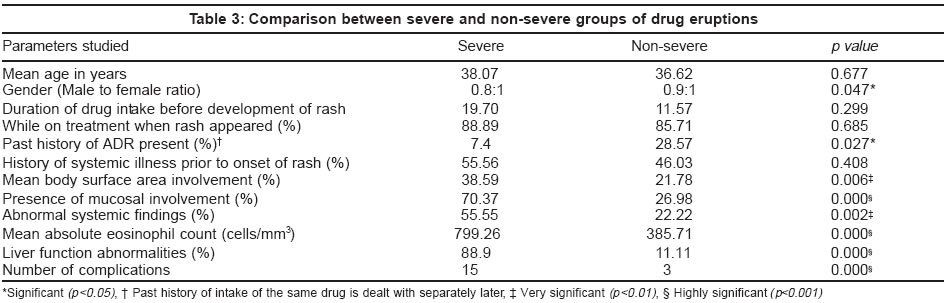
Indian Journal of Dermatology, Venereology, Leprology, Vol. 70, No. 1, January-February, 2004, pp. 20-24 Studies Adverse cutaneous drug reactions: Clinical pattern and causative agents in a tertiary care center in South India Pudukadan David , Thappa Devinder Mohan Department of Dermatology and STD, Jawaharlal Institute of Postgraduate Medical Education and Research (JIPMER), Pondicherry - 605006 Code Number: dv04005 ABSTRACT Background: Adverse cutaneous drug reactions (ACDRs) are caused by a wide variety of agents. Aims: Our objective was to ascertain the clinical spectrum of ACDRs and the causative drugs in this part of India and to find any risk factors. Methods: Ninety patients with adverse cutaneous drug reactions were recruited for this study during 2001-2003. Hematological and biochemical investigations were done in all of them. The VDRL and HIV (ELISA) tests were performed where the underlying risk factors were present. Patch testing, intradermal testing and oral provocation tests were done wherever feasible. Results: The mean age of the patients with cutaneous drug eruptions was 37.06 years. Most of them (52.2%) were in the age group of 20-39 years. The male to female ratio was 0.87: 1. The most common eruptions observed were fixed drug eruption (31.1%) and maculopapular rash (12.2%), and the most common causes were co-trimoxazole (22.2%) and dapsone (17.7%). Conclusion: The pattern of ACDRs and the drugs causing them is remarkably different in our population. Knowledge of these drug eruptions, the causative drugs and the prognostic indicators is essential for the clinician. INTRODUCTION Adverse cutaneous drug reactions (ACDRs) are responsible for approximately 3% of all disabling injuries during hospitalization. Many of the commonly used drugs have reaction rates over 1%.[1] There is a wide spectrum of cutaneous adverse drug reactions varying from transient maculopapular rash to fatal toxic epidermal necrolysis (TEN).[2],[3] The pattern of cutaneous adverse drug eruptions and the drugs responsible for them keep changing every year. The objective of our study was to ascertain the clinical spectrum of ACDRs and the causative drugs, and to find any risk factors in a tertiary care center in South India. METHODS Ninety consecutive patients with adverse cutaneous drug reactions were recruited for this study during 2001-2003. Reactions where the drugs taken were not known were excluded. The detailed history (including age, sex, duration of eruption, drugs responsible and complications) and physical examination findings were recorded. Hematological and biochemical investigations (serum electrolytes, blood sugar, liver and renal function tests) were done in all cases. The VDRL test and HIV (ELISA) test were performed where the underlying risk factors were present. For patch testing, the standard concentration of the incriminated agent was dispersed in a suitable vehicle and applied using a Finn chamber on the lateral aspect of the upper arm. The reaction was observed after 48 hours. The reading was graded based on International Contact Dermatitis Group (ICDRG) recommendations.[4] Intradermal testing and oral provocation tests were done as per the standard protocol wherever feasible and ethical as per our institute′s Ethical Committee recommendations. The severity of the reaction was graded according to the University of Virginia Health System Adverse Drug Reaction Reporting Program criteria as follows:[5] The data were analyzed utilizing Chi square test and independent ′t′ test. RESULTS The mean age of our patients with cutaneous drug eruptions was 37.06 years (± 30.12; range, 9-75 years). Most of them (47/90) were in the age group of 20-39 years, followed by 22 patients in the 40-59 years age group, 11 in the 60-79 years age group, and 6 in the 0-19 years age group. The male to female ratio was 0.87:1. The major presenting complaint was symptomatic rash (56.7%; 51/90 patients), followed by blistering (22%; 20/90) and pustular rash in (3.3%; 3/90). The mean duration of intake of medicine prior to the onset of the drug rash was 14.01 days (± 24.45; 1-172 days). Most of the cases (86.7%; 78/90 cases) developed a rash while they were taking the incriminated drug. Of the 90 consecutive patients, 25 had consumed the same drug earlier, 13 had a similar cutaneous reaction earlier and 12 had no reactions. A history of premarital/extramarital sexual exposure was obtained in 8.9% (8/90) of patients; only one patient was HIV seropositve, and all these patients were VDRL non-reactive. A history of a previous systemic illness was present in 44 patients (48.9%); 12 (13.3%) had a major illness while the remaining 32 (35.6%) had a minor one. Most of our patients (41/90) had 0-10% body surface area involvement; 31 patients had 31-90%, 15 had 11-30%, and just 3 had more than 90% body surface area involvement. About 40% of the patients (36/90) had mucosal involvement. Systemic manifestations were present only in 32.2% (29/90). Eosinophilia (absolute eosinophil count > 500 cells/mm3)[6] was present in 42.2% of patients (38/90) and liver function abnormalities in 23.3% (21/90). Only 10% In 87 of the 90 patients the suspected drug was withdrawn and the skin lesions subsided in 90.8% (79/87 cases) of them. Rechallenge (with griseofulvin, methotrexate, diclofenac sodium and co-trimoxazole in 1 case each) was done only in the four cases in whom the dechallenge results were doubtful or negative, and was positive in all of them. Patch testing was undertaken in 11 patients; most (8/11; 72.7%) gave positive results. Mild adverse cutaneous reactions were observed in 42.2% (38/90) cases, moderate adverse cutaneous reactions in 27.7% (25/90), and severe disease in 30% (27/90). The various types of drug eruptions are shown in [Table - 1] and the commonly implicated drugs in [Table - 2]. Correlation of the severity of the drug eruption with various clinical parameters is tabulated in [Table
- 3]. For the purpose of analysis, the patients were divided into 2 groups based on severity, i.e. severe and non-severe. The non-severe group included both mild and moderately severe cases of drug eruptions [Table
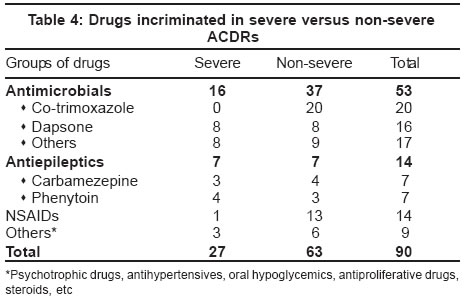
- 4]. The mean body surface area involvement was 38.5% (± 29.4; 6-96%) in the severe group compared to the 21.7% (± 24.31; 1-90%) in the non-severe group. Abnormal systemic findings were observed in 55.5% Complications were seen in 18 of the 90 patients of drug eruptions, mostly in SJS (6/7 patients) and TEN (5/9 patients), and included septicemia (6), urinary tract infections (3), ocular involvement (2), oral candidiasis (2), renal involvement (2) and balanoposthitis (1). Two patients died while on treatment. DISCUSSION Adverse cutaneous drug reactions vary in their patterns of morphology and distribution. In previous studies the most common morphologic patterns are exanthematous, urticarial and/or angioedema, fixed drug eruption and erythema multiforme.[7] Of the various types of ACDRs seen in our study, fixed drug eruption (FDE) was the most common drug eruption (31.1%), followed by maculopapular rash (12.2%). Others have noted exanthematous eruption to be most common type of drug eruption.[9],[10] A study from North India also found maculopapular rash to be most common type of ACDR.[3] This variation could be due to different patterns of drug usage and different ethnic group characteristics. Commonly incriminated drugs in our study were co-trimoxazole (22.2%), followed by dapsone (17.8%), phenytoin (7.8%) and carbamazepine (7.8%). Our institution is located in an area endemic for leprosy and, besides leprosy, dapsone is being used for many other dermatoses like lichen planus, bullous pemphigoid, etc. This could possibly explain the number of cases of dapsone induced adverse cutaneous drug eruptions seen in our hospital. Dapsone and antiepileptics were more commonly incriminated in severe drug eruptions, whereas cotrimoxazole and NSAIDs were more commonly involved in non-severe drug eruptions. When we looked at the drugs in broad groups, antimicrobials formed the major group (58.88%), followed by antiepileptics and NSAIDs (15.55% each). This is in concordance with an earlier report from North India.[3] Antimicrobials, followed by NSAIDs and central nervous system depressants were the most common implicated drugs in another study.[10] We observed a slight predominance of female patients. All cases of acneiform eruptions were reported in female patients, possibly because women are more conscious of this relatively asymptomatic eruption. Men seemed to predominate in cases of eczematoid drug eruptions, exfoliative drug eruptions, psoriasiform drug eruptions, maculopapular drug eruptions and fixed drug eruption. The majority our patients belonged to the 20-39 years age group, as also observed in another Indian study.[3] Another study observed that adults aged 20-49 years were at greatest risk of antibiotics-related drug eruptions, probably due to increased exposure to antibiotics.[11] However, two other studies noted that the elderly are more commonly affected.[12],[13] Adverse reactions to drugs increase with age.[9] This may be due to the increased use of medications by the elderly, increased potential for drug-drug interactions, and altered drug handling by the body. The difference in various studies may be related to the regional variation in the health care seeking behavior of the population.[3] Many of our patients (48.9%) gave a history of previous systemic illness. Multiple medical problems increase the chance of developing adverse drug eruptions.[13] Adverse drug reactions amongst pediatric patients are influenced by several factors like prolonged hospital stay, the classes of drugs used and polypharmacy.[14] This might be extrapolated to other age groups as well. We found visceral involvement predominantly in patients with SJS-TEN, exfoliative dermatitis, psoriasiform dermatitis and angioedema. Visceral involvement may predict a poor prognosis in SJS-TEN.[15],[16] It may be due to the drug eruption or it may be due to a pre-existing disease. The mean absolute eosinophil count was abnormal in most eruptions, with values more than 500 cells/mm3, except in cases of acneiform eruptions, urticaria/angioedema, and eczematoid, lichenoid and fixed drug eruption patients. Higher mean eosinophil counts were seen in the severe types of drug eruptions. Various textbooks[7] state that an elevated peripheral eosinophil count is an uncommon finding in cutaneous drug eruptions and therefore, contrary to the popular belief, its presence or absence is of little importance in excluding or confirming the diagnosis. According to Romagosa et al,[17] a peripheral eosinophil count carries little diagnostic value in the setting of adverse cutaneous drug eruptions. Guidelines of the American Academy of Dermatology state that eosinophil counts more than 1000 cells/mm3 indicate a serious drug-induced cutaneous eruption.[18] In our study, the absolute eosinophil counts were consistently higher in the so-called serious adverse cutaneous reactions. Although described as a test of little diagnostic value, absolute eosinophil counts may be useful in assessing the prognosis early in the disease course. Abnormal liver function tests also have been described as an independent indicator of the severity of a drug-induced cutaneous eruption.[18],[19] To conclude, the pattern of ACDRs and the drugs causing them are remarkably different in our population. A sound knowledge of these drug eruptions may help the clinician to better manage their cases. REFERENCES
Copyright 2004 - Indian Journal of Dermatology, Venereology, Leprology The following images related to this document are available:Photo images[dv04005t2.jpg] [dv04005t4.jpg] [dv04005t3.jpg] [dv04005t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}