 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
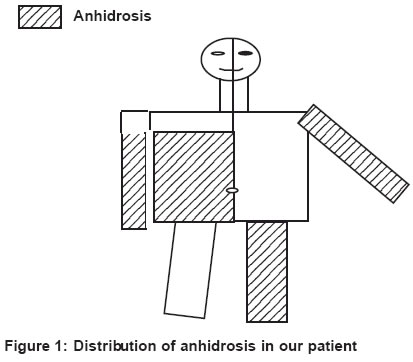
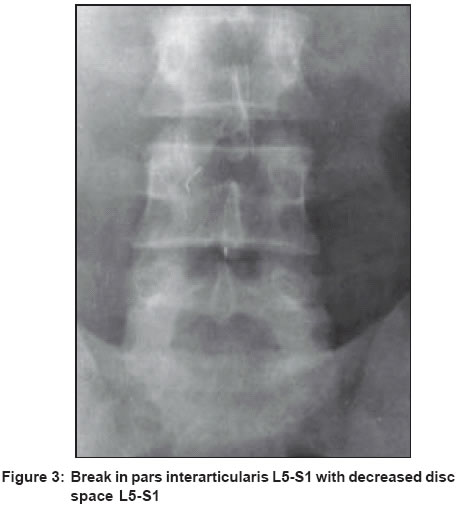
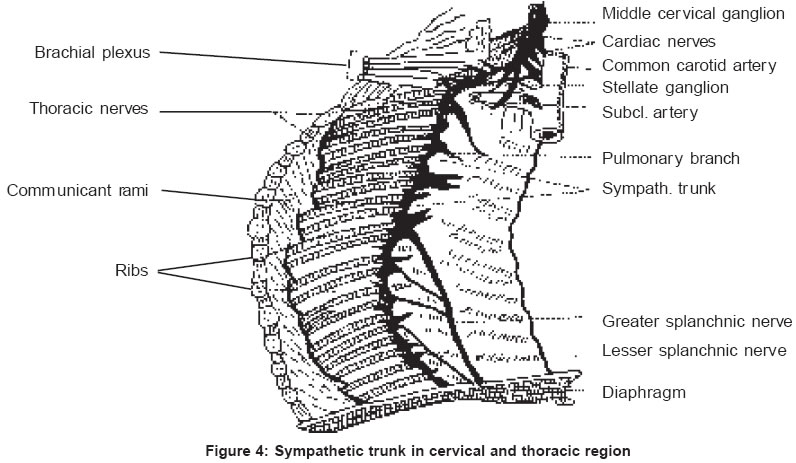
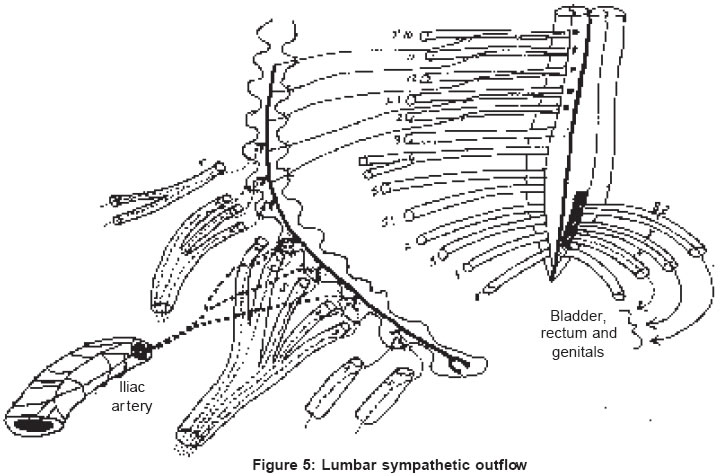
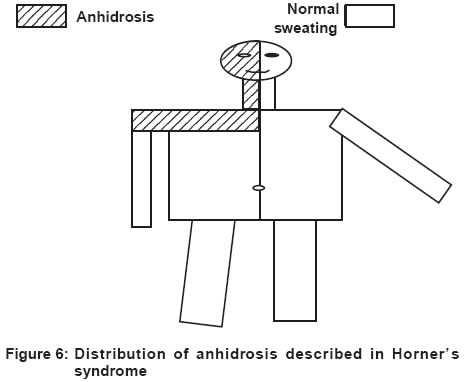
Indian Journal of Dermatology, Venereology, Leprology, Vol. 70, No. 1, January-February, 2004, pp. 29-32 Case Report Segmental anhidrosis with hyporeflexia associated with congenital spinal deformity: A Ross’s syndrome variant or inverse Horner’s syndrome? Sawhney MPS, Sharma YK, Singh N Department of Dermatology and STD Command Hospital (SC), Pune - 411040 Code Number: dv04007 ABSTRACT A 39-year-old soldier presented with anhidrosis affecting both upper extremities below the shoulders, the right side of the trunk below the third rib in front and the third vertebra on the back, and the left lower extremity below the inguinal ligament since 1992. Ten years later in 2002, he was also found to have bilateral absence of Achilles reflex and decreased right knee jerk. In addition, the patient was found to have congenital spinal abnormalities in the form of block of vertebrae C3-C4; decreased disc space C4-C5; and break in pars interarticularis L5-S1 with decreased disc space. A total of seven cases of Ross syndrome, Holmes-Adie syndrome (tonic pupil with lost tendon jerks) with segmental anhidrosis, have been described in the literature. Our case, however, did not have any pupillary abnormality. A case of progressive isolated segmental anhidrosis has also been described. The association of congenital spinal abnormality, which may be pathognomonic in the causation of this progressive sudomotor degeneration, is quite interesting in our case. The distribution of anhidrosis on the right side is just below the level of sweating loss sometimes described in lesions of superior sympathetic cervical ganglion in Horner’s syndrome.INTRODUCTION In 1958, Ross described for the first time a case of tonic pupil and areflexia of the lower extremities (Holmes-Adie syndrome) and segmental hypohidrosis.[1] Only a few such cases have subsequently been reported in the literature.[2],[3],[4],[5],[6],[7] The progressive abnormality of sweating is probably due to sudomotor denervation and the associated Holmes-Adie syndrome was thought to be coincidental. Horner′s syndrome, on the other hand, occurs due to lesions of the superior cervical sympathetic ganglion and leads to a constricted pupil with absence of dilatation, drooping of the upper eyelid, absence of ciliospinal reflex and, less commonly, anhidrosis on the corresponding half of the face and neck up to the 3rd rib and the 3rd thoracic spine and the upper limb on the same side.[8] We report here a case of anhidrosis of both upper extremities, right half of the trunk and lower extremity, associated with hyporeflexia in both lower extremities with an association of congenital deformity affecting both the cervical and the lumbar spines. CASE REPORT A 39-year-old soldier presented with complaints of absence of sweating in the upper limbs, right side of the trunk and left lower limb with excessive sweating on the rest of the body since 1992. He gave a history of a self-limiting episode of syncope during a long distance run. However, in 1993, while posted in a desert area he developed intolerance to heat and was hospitalized; a detailed check up, including a neurological examination, was normal. A skin biopsy ruled out anhidrotic ectodermal dysplasia, since the number of sweat glands was normal . He was diagnosed as having localized idiopathic anhidrosis and placed under observation. In 1995, on MRI scan the patient was found to have block vertebra C3-C4 with a normal spinal cord and the diagnosis was changed to idiopathic acquired anhidrosis. There was no history of trauma or any prolonged febrile illness. Repeated blood pressure readings (lying and standing) did not show any significant difference. Head up Tilt Test (HUTT) showed normal study with good orthostatic tolerance. The pupils were horizontally oval but dilated fully with mydriatic drops and became circular. Ankle jerks were absent on both sides and knee jerks were reduced on the right side. Dermatological examination revealed the absence of sweating and raised temperature in both upper limbs below the shoulders, the right side of the trunk below the third rib in the front and the third spine behind, and the left lower limb below the inguinal ligament [Figure - 1]. A radiograph of the cervical spine reconfirmed block vertebra C3-C4 with osteophytic changes in C4 and C5 and decreased disc space between C4-C5 [Figure - 2]. A radiograph of the lumbosacral spine showed a break in pars interarticularis of L5-S1 with decreased disc space [Figure - 3]. Pilocarpine test with 1:1000 solution showed no sweating in the anhidrotic area as compared with the normal control. The patient was diagnosed as a case of segmental anhidrosis with compensatory hyperhidrosis, associated with lost/decreased tendon jerks in the lower extremities and congenital spinal deformity, in the absence of any significant pupillary abnormality or orthostatic hypotension. DISCUSSION Anhidrosis can be observed in a wide variety of neurological and dermatological disorders. Segmental distribution of anhidrosis, normal skin biopsy, normal MRI scan of the spinal cord, absence of other manifestations of peripheral neuropathy and absence of sweating in the anhidrotic areas on pilocarpine test confirmed it to be a case of an autonomic dysfunction involving the postganglionic sudomotor cholinergic sympathetic nerve fibres.[5] In contrast to Ross′s syndrome, our patient did not have any significant pupillary abnormality but did have loss of tendon jerks in the lower limbs. In all previously reported cases except one, the onset of tonic pupil preceded that of anhidrosis by months to years.[1],[2],[3],[4],[5],[6] Hardin and Gay described a case whose anhidrosis may have preceded tonic pupil by six years, but the absent tendon reflexes were noted nine years before the onset of anhidrosis.[4] However, as in our case, Faden et al have described a case of progressive isolated segmental anhidrosis without any pupillary abnormality or lost tendon jerks.[9] Other autonomic dysfunctions like orthostatic hypotension have also been described in association, thereby suggesting that there can be a widespread dysfunction of the sympathetic nervous system in these cases.[7] The association of a congenital anomaly involving the cervical as well as the lumbosacral spine has not been reported earlier. Involvement of the stellate ganglion on both sides (causing anhidrosis of the upper limbs), the upper thoracic ganglion on the right side (causing anhidrosis on the right side of the trunk), and the left lower thoracic and lumbar sympathetic ganglia (causing anhidrosis of the left lower extremity), some of them overlying the above congenital spinal deformity, may be pathognomonic [Figure - 4] and [Figure - 5]. Further, the anhidrosis on the right side of the trunk and the upper extremity is just below what has been described in Horner′s syndrome, which is due to a lesion of the superior the cervical ganglion [Figure - 6].[8] Hence, it will not be incorrect to say that our patient had inverse Horner′s syndrome on the right side. REFERENCES
Copyright 2004 - Indian Journal of Dermatology, Venereology, Leprology The following images related to this document are available:Photo images[dv04007f6.jpg] [dv04007f5.jpg] [dv04007f3.jpg] [dv04007f4.jpg] [dv04007f1.jpg] [dv04007f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}