 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
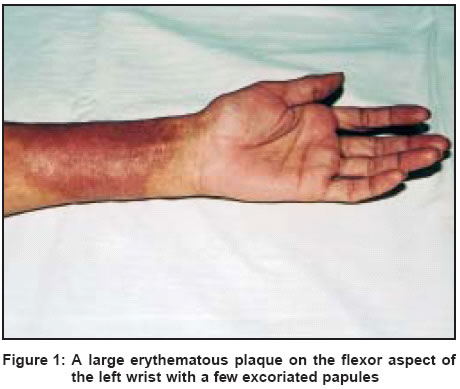
Indian Journal of Dermatology, Venereology, Leprology, Vol. 70, No. 1, January-February, 2004, pp. 33-35 Case Report Dermatitis recall during disulfiram therapy Zawar Vijay , Nerlikar Shobha Consultant Dermatologist, Nashik Code Number: dv04008 ABSTRACT We report an alcoholic Indian man, a known case of contact dermatitis to nickel, who presented with recurrence at the same site, without having recent contact with nickel, following disulfiram therapy for his alcohol addiction.INTRODUCTION Disulfiram is an important drug in the supportive therapy of alcohol addiction.[1] Several cutaneous reactions to this drug have been described.[2],[3] Disulfiram reactions in nickel sensitive individuals are known.[4],[5],[6] We came across a patient whose nickel dermatitis was exacerbated following disulfiram therapy. CASE REPORT A 43-year-old businessman was hospitalized for the treatment of alcohol addiction of 15 years′duration and was treated with oral disulfiram 0.75 g/day. On day 4 of therapy, he developed an acute intensely pruritic rash on his left wrist. He had not consumed alcohol since five days. He gave a history of having developed a similar rash at the same site twice earlier. The first time was 15 years back when he was diagnosed to have contact dermatitis to the nickel in the new metal belt of his wrist-watch. On subsequent patch testing he had tested positive for nickel sulfate. Since then he had stopped using a wrist-watch and was very diligent in handling metallic objects. The second instance was 5 years earlier when he had been hospitalized for alcohol de-addiction and had been given disulfiram 0.5 g/day orally. On the third day of treatment he had developed a rash which spontaneously resolved after a few hours. History of contactants at work or at home, hobbies or belongings, and occupational and dietary histories did not point to any obvious source of exposure to objects containing nickel, rubber or cobalt. There was no recent history of any suspicious objects coming particularly in contact with the left wrist. There was no history of using any topical applications prior to the onset of the eruption. There were no other relevant cutaneous lesions elsewhere on the body. At the time of admission (before disulfiram therapy), he had bilateral palmar erythema and onychomycosis of both great toenails; no treatment was sought for these conditions. His past health was good and he was not a known diabetic or hypertensive. His general and systemic examinations were normal. Dermatological examination revealed a large erythematous plaque with slight edema encircling the left wrist, about two centimeters distal to the wrist joint, and more marked on the flexor aspect [Figure - 1]. Also seen were a few scattered erythematous papules at the periphery of the plaque, some excoriated. His baseline work up, including complete blood count, blood sugar, and urinalysis, was normal. The VDRL and HIV (ELISA) tests were non-reactive. His liver function tests were normal except for a marginal rise in the SGPT level (60 IU/dl). Skin biopsy and patch testing were not done. The patient believed that his skin problem was a drug reaction to disulfiram, but upon our assurance he continued disulfiram therapy. He was prescribed betamethasone dipropionate cream 0.05% for local application twice a day and hydroxyzine hydrochloride tablets orally, 10 mg twice a day. His eruption completely resolved within five days despite continuing disulfiram. DISCUSSION Klein and Fowler in 1992 reported a similar case of the recall of dermatitis on the wrist and the abdomen after disulfiram therapy, despite the patient having no recent contact with nickel in the watchstrap and the belt buckle.[5] A similar case was also reported by Gamboa et al.[6] Materials containing thiuram have also been reported to induce such reactions during disulfiram therapy in patients known to have contact dermatitis due to rubber.[4] Dermatitis due to cobalt has also been reported to be exacerbated during disulfiram therapy.[7] Disulfiram is known to result in the chelation of metals such as nickel. The effects of disulfiram on nickel metabolism involve chelation of dietary nickel by diethyldithiocarbamate (DDC), a disulfiram metabolite. It causes nickel stores inside the body to get mobilized and is associated with a rise in the urinary and serum levels of nickel, mimicking the challenge with oral nickel. The latter results, in turn, in a flare of dermatitis at the sites of nickel induced contact dermatitis experienced earlier in life, in the absence of repeat contact with nickel.[5] Hence, the resultant dermatitis is aptly described as "dermatitis recall". This property of disulfiram to reduce nickel in the body has led to its evaluation as a treatment for recalcitrant cases of contact dermatitis due to nickel.[8] Kaaber et al reported exacerbation of dermatitis in 9 of 11 patients after 1 to 7 days of starting disulfiram therapy for nickel-induced eczema. Interestingly, such flare ups are said to be more severe than those caused by an actual oral challenge with nickel.[5],[8] Though the location and the presentation were typical in our patient, we were initially puzzled because there was no history of recent contact with nickel items. Disulfiram implants are also reported to induce allergic cutaneous reactions[9] and it is a matter of concern whether our patient would be more prone for such unusually severe dermatitis as he needs insertion of a disulfiram implant. We believe that it is mandatory that a history of nickel and rubber contact dermatitis be recorded before starting disulfiram therapy. Likewise, physicians who use disulfiram for treating alcohol addiction should advise patients who have had contact dermatitis to nickel, rubber or cobalt in the past to avoid contact with objects containing these materials. In conclusion, dermatitis recall is an uncommon phenomenon, which could be alarming in patients receiving disulfiram for alcohol abuse. It may result in the patient deferring further treatment thinking that it is a drug eruption. Hence, physicians involved in the treatment of alcohol abuse should be aware of this condition while treating nickel-sensitive patients with disulfiram. Such patients, in turn, should be warned beforehand about the possibility of recall of dermatitis during therapy even if the relevant contactant is avoided. REFERENCES
Copyright 2004 - Indian Journal of Dermatology, Venereology, Leprology The following images related to this document are available:Photo images[dv04008f1.jpg] |
| |||||||||

{kind=link}