 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
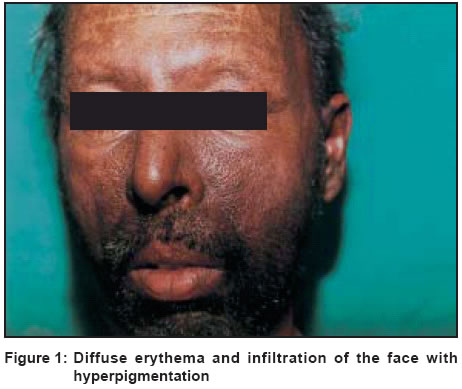
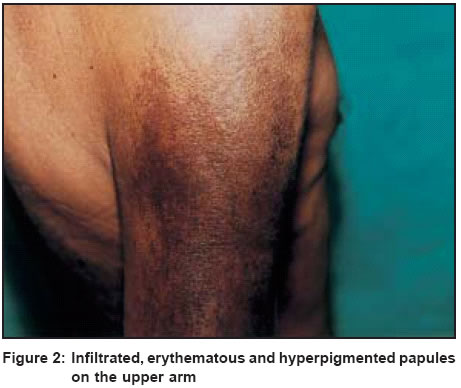
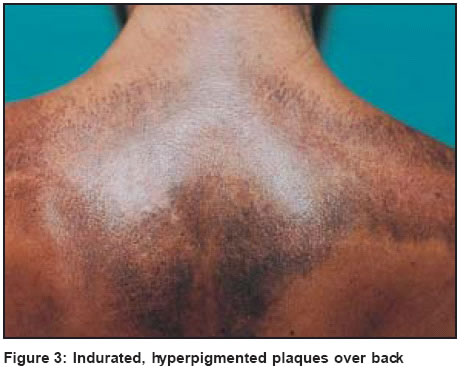
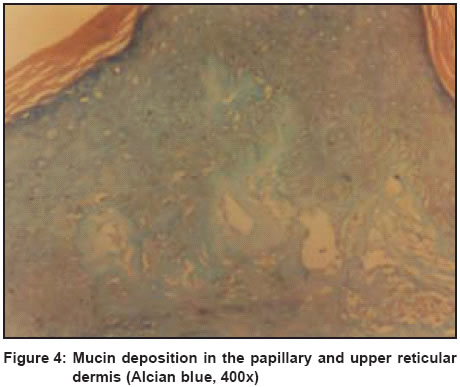
Indian Journal of Dermatology, Venereology, Leprology, Vol. 70, No. 1, January-February, 2004, pp. 36-38 Case Report Scleromyxedema with subclinical myositis Prasad PVS, Joseph Joe Mathew , Kaviarasan PK, Viswanathan P Department of Dermatology, Venereology and Leprosy, Rajah Muthiah Medical College and Hospital, Annamalai University, Annamalai Nagar Code Number: dv04009 ABSTRACT A 49-year-old farmer presented with papules on the face, arms, chest and back associated with sclerosis. Histopathology and PAS stain confirmed the clinical diagnosis of scleromyxedema. He also had elevated CPK levels due to myopathy. Screening for internal malignancy was negative.INTRODUCTION Lichen myxedematosus is a cutaneous myxedematous state characterized by the formation of numerous lichenoid papules which coalesce together to form generalized plaques, causing extensive thickening and hardening of the skin.[1] The disease usually affects adults between 30 and 50 years of age. Cardiovascular abnormalities can occur in 10% of cases. Others may complain of extreme muscular weakness and lassitude due to myopathic or neurological involvement.[2] Paraproteinemia is commonly found in spite of normal serum proteins. There is an elevation of IgG k light chain with mobility moving to the cathode.[3] Histopathology of the skin lesion reveals large amounts of mucin. The mucinous infiltrate is pronounced in the upper dermis and is associated with an increase in fibroblasts and collagen. The collagen bundles in the upper dermis are arranged irregularly.[4] There is a wide range of treatment alternatives that are only partially acceptable because of lack of therapeutic efficacy or because of severe complications. They are prednisone, cyclophosphamide, melphalan, isotretinoin, intravenous immunoglobulins, thalidomide, homologous bone marrow transplant and extracorporeal photochemotherapy.[2] CASE REPORT A 49-year-old male farmer complained of hyperpigmented skin lesions of 3 years′ duration and puffiness of face of one month′s duration. He initially noticed darkening of the skin on the face which progressively involved the upper chest, upper back and upper arms. Pruritus was moderate. At the same time, the patient also noticed a papular eruption on these sites. One month prior to his visit to the hospital, he noticed puffiness of the face. There was no history of atopy, extra-marital sexual exposure, photosensitivity or systemic complaints. On examination there was no pallor, cyanosis, clubbing or pedal edema. The axillary lymph nodes were palpable bilaterally, and were firm and nontender. The pulse rate, blood pressure, systemic examination, genitalia and per rectal examination were all within normal limits. Cutaneous examination revealed multiple infiltrated plaques over the face, neck anterior chest wall, interscapular region, back and upper limbs [Figure - 1], [Figure - 2], [Figure - 3]. There was puffiness of the face and inability to retract the lower eyelids. The skin was bound down at these sites. There were also hyperpigmented papules over the face, neck, scalp and back. The forehead creases were spared. The scalp showed diffuse alopecia. The palms, soles, nails and mucosa were normal. A clinical diagnosis of scleromyxedema was made and the patient was further investigated. The hemoglobin was 8 g%, the ESR was normal, the total and differential white blood count were normal, and the platelet count was 1,00,000 cells/cmm. The peripheral smear revealed a normocytic normochromic anemia. The urine was normal and there was no occult blood in the stool. The blood sugar, and renal function tests and thyroid function tests were normal, but the liver function tests revealed increased aspartate aminotransferase (70 U/L) and alanine aminotransferase (80 U/L) levels. The serum alkaline phosphatase was 149 U/L and the serum creatinine phosphokinase (CPK) was 247 U/L. The twenty four hours urinary protein estimation and ultrasonography of the abdomen were normal. A chest X-ray and electrocardiogram were within normal limits. ELISA for HIV screening was negative. The serum electrophoretic pattern revealed a relative increase in gamma globulin, i.e. 1.3 U/L (normal 0.5 - 1 U/L). Electromyography (EMG) from the right deltoid muscle showed prolonged insertional activity, few fibrillation potentials and incomplete interference pattern with short duration, low amplitude polyphasic units. All these features were suggestive of myositis. A skin biopsy revealed mucin deposition in the upper dermis which was confirmed by an Alcian Blue stain [Figure - 4]. The findings of a biopsy from the right deltoid muscle were consistent with myopathy. The patient was started on combination therapy with cyclophosphamide 50 mg twice a day and oral prednisolone 40 mg per day. Prednisolone was tapered to 20 mg after one month. With this combination therapy the patient subjectively improved and the papules improved by 75% after one month. Both the drugs are being continued and the patient is being regularly followed-up. DISCUSSION Our patient was diagnosed to have scleromyxedema on the basis of chronicity of skin lesions, a generalized papular and sclerodermoid eruption, and mucin deposition, fibroblast proliferation and fibrosis on histopathology with normal thyroid function tests. Extensive screening did not reveal any internal malignancy. The serum creatinine phosphokinase was raised and this was confirmed by serial estimations. Electromyography and muscle biopsy revealed myopathy but there was no clinical evidence of myositis. Scleromyxedema may be associated with various underlying conditions like neurological events, scleroderma, atherosclerosis, dermatomyositis, multiple keratoacanthomas and an underlying carcinoma.[5] Launay described a 41-year-old man with scleromyxedema and dermatomyositis.[6] Slight to severe proximal muscle weakness is found in 27% of patients and occasionally associated with slight elevation of muscle enzymes and inflammatory electromyographic findings. Thus our patient had an interesting association of increased muscle enzymes and myopathy with scleromyxedema in the absence of clinical evidence of myositis. Our patient had increased gamma globulin levels but we could not investigate this further to learn if it was a monoclonal spike and moved toward cathode which could have supported our diagnosis. REFERENCES
Copyright 2004 - Indian Journal of Dermatology, Venereology, Leprology The following images related to this document are available:Photo images[dv04009f3.jpg] [dv04009f4.jpg] [dv04009f2.jpg] [dv04009f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}