 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
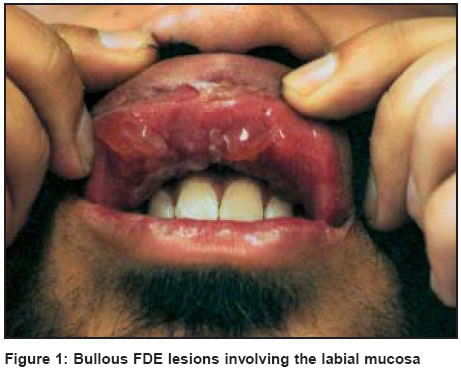
Indian Journal of Dermatology, Venereology, Leprology, Vol. 70, No. 1, January-February, 2004, pp. 44-45 Letter To Editor Nimesulide induced bullous fixed drug eruption of the labial mucosa Kumaran Sendhil , Sandhu Kamaldeep , Saikia Uma Nahar , Handa Sanjeev Departments of Dermatology, Venereology & Leprology, Post graduate Institute of Medical Education and Research, Sector 12, Chandigarh Code Number: dv04013 Sir, A fixed drug eruption (FDE) is a distinct drug induced reaction pattern that characteristically recurs at the same skin or mucosal site. We report a case of bullous FDE confined to the labial mucosa following intake of nimesulide, a commonly used nonsteroidal anti-inflammatory drug in India. A 23-year-old man presented with multiple oral blisters of one day′s duration associated with marked burning and soreness. He had developed the lesions within 5 to 6 hours of taking a single tablet of nimesulide (which he had taken by himself). He had also been taking roxithromycin for three days which had been prescribed for his sore throat by an otolaryngologist. In the past he had taken multiple courses of roxithromycin for his recurrent sore throat without any complaints, but this was the first time that he had taken nimesulide. The patient was afebrile and there were no other associated systemic complaints. Examination revealed multiple, tense bullae filled with clear fluid, varying in size from 0.5-1.5 cm, distributed over the upper labial mucosa with slight surrounding erythema [Figure - 1]. The rest of the oral mucosa and other mucosal sites were free of lesions. A biopsy from the bullae was taken. Histopathological examination revealed necrotic keratinocytes and a marked inflammatory infiltrate in the dermis, findings consistent with a fixed drug eruption. The patient was asked to stop both the drugs and to avoid nimesulide in the future. He was given a short course of steroids in a tapering dose for two weeks following which the lesions improved. The lesions healed with mucosal hyperpigmentation. Brocq first introduced the term fixed drug eruption in 1894.[1] The pathogenetic mechanism underlying FDE is still enigmatic. The most commonly accepted hypothesis is persistence of memory T cells in the affected skin.[2] CD8+ cells phenotypically resembling effector memory T cells have been shown to be greatly enhanced in the lesions of FDE.[3] The lesions of FDE usually start as an erythematous macule that subsequently evolves into a plaque. Vesicles and bullae develop at a later stage and are usually hemorrhagic. The lesions can occur on any part of the skin and mucous membranes. The sites of predilection are the limbs, sacral region, genitalia, palmar and plantar skin. The oral mucosa may be involved in association with skin lesions or alone. The drugs that commonly cause mucosal FDE include co-trimoxazole, oxyphenbutazone, and tetracycline.[4] Classically the transitional epithelium of the mucocutaneous junctions is involved but strict localization of the lesion to the labial mucosa, as was seen in our patient, is unusual. Systemic manifestations are uncommon and include fever, malaise, nausea, diarrhea, abdominal pain, urethritis, and conjunctivitis. Nimesulide is a nonsteroidal anti-inflammatory agent with antipyretic and analgesic properties. It is being commonly prescribed in India.[5] Some of the side effects reported with its use are pruritus, urticaria, purpura, maculopapular rash and localized toxic pustuloderma.[6],[7] Due to severe hepatotoxicity and hemolytic anemia associated with its use, nimesulide is likely to be withdrawn from the market in many countries.[8] To the best of our knowledge only 8 cases of FDE secondary to nimesulide have been reported[9],[10],[11],[12] and there is only one other report with primarily oral mucosal involvement.[9] This report emphasizes an uncommon mucosal localization of bullous FDE due to nimesulide. REFERENCES
Copyright 2004 - Indian Journal of Dermatology, Venereology, Leprology The following images related to this document are available:Photo images[dv04013f1.jpg] |
| |||||||||

{kind=link}