
|
Indian Journal of Dermatology, Venereology and Leprology
Medknow Publications on behalf of The Indian Association of Dermatologists, Venereologists and Leprologists (IADVL)
ISSN: 0378-6323 EISSN: 0973-3922
Vol. 70, Num. 2, 2004, pp. 67-75
|
Indian Journal of Dermatology, Venereology, Leprology, Vol. 70, No. 2, March-April, 2004, pp. 67-75
Review Article
Therapeutic options for systemic sclerosis
Akerkar Shashank M, Bichile Lata S
Dept. of Rheumatology, Seth GS Medical College and KEM Hospital, Mumbai
Correspondence Address:Dept. of Rheumatology, Seth GS Medical
College and KEM Hospital, Mumbai lsbichile@rediffmail.com
Code Number: dv04022
ABSTRACT
Systemic sclerosis is a uncommon connective tissue disorder characterized by vascular damage, immune cell activation and fibrogenesis. Each of these components may respond to different therapies. Therefore, a combination strategy treating all three processes is more likely to control the disease than single agent therapy. Clinical trials have gone a long way towards defining the therapy of scleroderma and many drugs previously used for scleroderma have been critically assessed. Angiotensin blockade is effective in treating as well as preventing scleroderma renal crisis. The 9-year cumulative survival has improved from 38% to 68% after the introduction of angiotensin blockade. There is definitive evidence supporting the use of cyclophosphamide in systemic sclerosis associated alveolitis. Newer molecules aimed at various cytokines are being tried. The therapy for systemic sclerosis is far from perfect at present. But, individualization of the treatment with respect to stage and subset of disease as well as organ involvement can eventually result in rational, effective management.
INTRODUCTION
Systemic sclerosis is an uncommon acquired connective tissue disorder characterized by an abnormal thickening of the skin. It is a multisystem disease with overproduction of collagen, widespread vascular damage with the development of microvascular obliteration, and tissue infiltration of mononuclear inflammatory cells. Though externally the skin seems to bear the brunt of the disease, internally various organs are equally affected by the same process.
Treatment concepts
The goals of treatment are:
- Prevent internal organ damage.
- Arrest or slow the deterioration of function in previously involved
organs.
- Improve the function of previously involved organs, including
the skin.
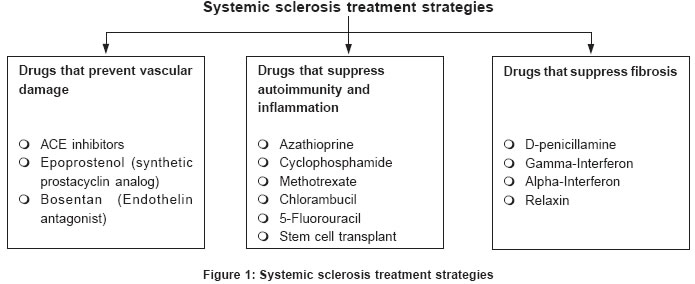
The three underlying processes in systemic sclerosis are vascular damage, immune cell activation and fibrogenesis. Each of them may respond to different therapies [Figure
- 1]. Therefore, a combination strategy treating all three processes is more likely to control the disease than single agent therapy.[1] Since endotheliopathy and vasospasm are features throughout the course in diffuse scleroderma and limited scleroderma, vascular therapies should be used in combination with other agents. Moreover, therapies must also be matched to the disease stage and subset. Thus, for early diffuse systemic sclerosis, immunosuppressive treatment is the most appropriate approach. At later stages, antifibrotic interventions are most important. Vasodilator intervention is important at all stages of the disease.
Status of established therapies for scleroderma
Clinical trials have gone a long way towards defining the therapy of scleroderma and many drugs previously used for scleroderma have been critically assessed. D-Penicillamine
This has been one of the most commonly used drugs in the management of systemic sclerosis due to its property of interfering with the cross linking of collagen, thus increasing the soluble collagen,[2] and a probable immunomodulatory effect. Since 1966, many studies have tried to assess its efficacy,[3],[4],[5],[6],[7],[8],[9],[10],[11],[12],[13],[14] but they have been uncontrolled, have used different dosages and durations, and have showed a wide spectrum of conclusions, varying from no effect to 70% favorable response. In 1982, Steen et al analyzed a large group of patients with early diffuse scleroderma.[12] In this retrospective study, D-penicillamine treatment was associated with significant improvement in the skin thickness, better survival and fewer instances of scleroderma renal crisis compared with a similar (non-randomized) comparison group receiving no treatment or other treatments. Twice as many patients had more than 25% improvement in skin score. New organ involvement was reduced and the 5-year cumulative survival rate was also higher in the penicillamine group. The drawback of this trial is that it did not have any randomized comparison group. Recently a large, randomized, double blind, multicenter study of D-penicillamine was conducted to compare low dose (62.5 mg daily) with high (conventional) dose (750 mg daily) therapy in patients with early diffuse systemic sclerosis (disease duration < 20 months).[15] It was expected that the conventional dose would be more effective than the low dose, but the skin scores in both the groups improved significantly and no dose response was observed. No difference was found in the mortality or the incidence of renal crisis in the two groups. This trial suggests that treatment with low doses of D-penicillamine is as effective as that with high doses, but it suffers from the disadvantage of not including controls. Thus conclusive data about the efficacy of D-penicillamine are still lacking. Methotrexate
Using a logical, but complex, definition of improvement, a trial showed a 63% improvement in 15 patients who were treated with methotrexate compared with a 10% improvement in 12 patients who were treated with placebo (p<0.05).[16] The study examined 29 patients with an average disease duration of 38 months. Another trial examined 71 patients who had diffuse scleroderma (median disease duration of 7 months).[17] The modified Rodnan skin score (MRSS) improved by 4.1 units in the patients who took methotrexate but worsened by 1.8 units in patients who took placebo (p<0.009). The UCLA skin score, which measures tethering, reached statistical significance (p<0.05). This trial showed trends to response without reaching statistical significance. Thus, the exact role of methotrexate as a disease-modifying agent in systemic sclerosis remains uncertain. Vasodilators
Two groups of vasodilators are available for use in scleroderma: calcium channel blockers and angiotensin converting enzyme (ACE) inhibitors (enalapril)/angiotensin receptor blockers (losartan). Both have an evidence-based benefit. However, when compared, nifedipine, a pure vasodilator, was less effective[18] or of no benefit[19],[20] in Raynaud′s phenomenon. A comparison of nifedipine vs. losartan also showed statistically better results with losartan.[21] Thus angiotensin converting enzyme inhibitors/angiotensin receptor blockers are more effective. Effects of angiotensin blockade: Angiotensin II is a profibrotic agent and induces collagen and fibronectin synthesis.[22],[23] It also stimulates transforming growth factor-beta (TGF-b) gene expression in fibroblasts and endothelial cells.[24],[25] Angiotensin converting enzyme inhibitors (ACEI) and angiotensin receptor blockers (ARB) block the pro-fibrotic renin angiotensin axis. Losartan also reduces the lung fibroblast proliferation and collagen production induction by angiotensin II in vitro.[26] Preliminary evidence also suggests that losartan not only improves Raynaud′s phenomenon but also beneficially modulates the levels of pro-collagen peptides and circulating isoforms of cell surface adhesion molecules.[27] Angiotensin-converting enzyme is also involved in the degradation of bradykinin, thereby regulating its effects on fibrinolysis and on platelet activation and aggregation.[28] Bradykinin, a potent vasodilator, reduces the production of tissue plasminogen activator and stimulates endothelial receptors that trigger prostacyclin and nitric oxide release.[29] ACEIs/ARBs are thus likely to have disease-modifying properties in addition to a vasodilator property, as is commonly believed. ACEIs reverse the scleroderma renal crisis.[30],[31] Retrospective studies already show that the 9-year cumulative survival has improved from 38% to 68% after the introduction of ACEIs in the management of scleroderma.[32] Thus, there is abundant evidence about the utility of ACEIs in scleroderma and the introduction of this group of drugs has resulted in a significant reduction in the mortality due to the disease. Corticosteroids
Corticosteroids are indicated only in inflammatory myositis,[33] the edematous phase of systemic sclerosis and for interstitial lung disease secondary to systemic sclerosis on a short term basis. The dosage of prednisolone used is 15-20 mg to avoid the long-term complications of steroids. One potential complication is their association with scleroderma renal crisis.[34],[35] High doses (prednisolone > 30 mg) have been proved to be a factor associated with the development of renal crisis.[36],[37] Pulse corticosteroids
Indian studies have shown the usefulness of pulse corticosteroid therapy in systemic sclerosis.[38],[39] An improvement in skin thickness, episodes of Raynaud′s phenomenon, pulmonary function, and calcinosis has been shown with pulse steroids (100 mg dexamethasone in 5% dextrose given intravenously for 3 days per pulse). In one study, the histopathological changes (perivascular mononuclear infiltrate, vessel wall changes, papillary dermis homogenization, and reticular dermis hyalinization) were evaluated in 8 patients with scleroderma on pulse dexamethasone. Although induration improved clinically, there was no consistent or uniform improvement in the various histopathological parameters.[40] Pulse steroid therapy in other dermatological diseases has been shown to be free of the common side effects of long term steroid therapy.[41] The question of pulse corticosteroid-induced osteoporosis remains unanswered as the trials looking for osteoporosis are limited to one or two pulses only.[42],[43],[44] However, role of pulse steroids remains questionable in view of reports regarding the causation of renal crisis with long-term high dose steroids. Cyclophosphamide
Cyclophosphamide has been used for patients with interstitial lung disease. Three trials have shown improvement in lung function with cyclophosphamide as compared to prednisone or D-penicillamine.[45],[46],[47] The largest series with 103 patients followed up over 13 months showed a median survival of 89% in those treated with cyclophosphamide compared to the 71% in the untreated group.[48] Thus there is definitive evidence supporting the use of cyclophosphamide in systemic sclerosis associated alveolitis and cyclophosphamide pulse therapy is regularly used for this indication in systemic sclerosis. Infliximab
Infliximab has been recently tried in scleroderma. It was combined with methotrexate in a patient with CREST syndrome and refractory ulcers with effective healing of the ulcers.[49] Minocycline
A recent study involved subjects with diffuse systemic sclerosis of less than 5 years duration who were treated with minocycline at a dose of 50 mg bid for one month followed by 100 mg bid for up to a year. Mean skin score improved only modestly in this study, the small degree of improvement (mean change in MRSS = -3.9 or 12.6%) was similar to that expected in the natural course of this disease.[50] Minocycline has also not been found to alter the metabolism of collagen 1 by dermal fibroblasts.[51] However, it may be useful in calcinosis associated with scleroderma.[52] Thalidomide
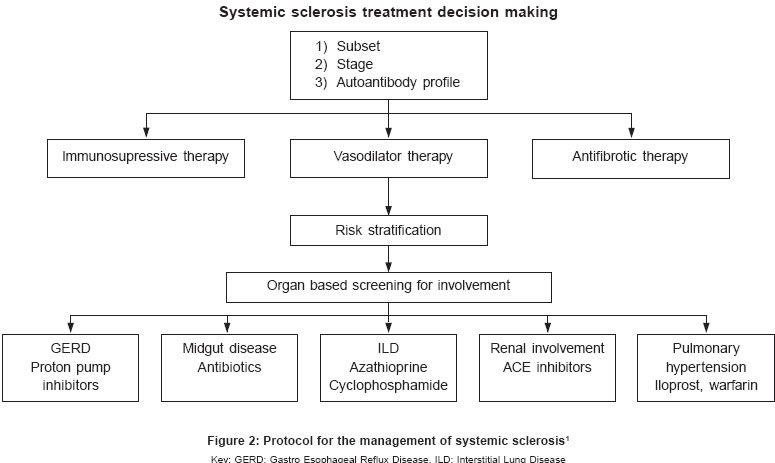
Thalidomide is a partial inhibitor of TNF-a production by LPS stimulated monocytes both in vitro and in vivo.[53],[54] Thalidomide seems to stimulate a Th-1 type of response.[55] The use of Thalidomide has been directed at the immunological component of scleroderma. A striking effect has been seen on extremity ulcers in scleroderma patients. Post treatment skin biopsies showed loosening of the collagen bundles and decrease in the thickness of the epidermal layer. Improvement was also seen in other symptoms like GE reflux but not in Raynaud′s episodes.[56] [Figure
- 2] shows a simplified protocol for the management of systemic sclerosis.
ORGAN BASED THERAPIES Effective management of systemic sclerosis consists of early detection of specific organ based complications. Specific organ based strategies are:
Management of critical digital ischemia
Digit threatening ischemia is characterized by severe pain and ischemic demarcation of the digit. Vasodilator therapy is maximized. For rapidly advancing ischemic lesion, anticoagulation with heparin is initiated. Low molecular weight dextran[57],[58] & pentoxyphylline infusion[59] have been tried with variable success. Prostacyclines have been a promising drug in this regard.[60] Epoprostenol, 0.5 to 2 ng/kg/min continuous infusion for 1 to 3 days or iloprost infusion at doses of 0.5 to 2.0 ng/kg/min can be administered daily for 1 to 3 days. When medical treatment fails, surgical interventions may be appropriate. Renal crisis
It is one of the major complications of systemic sclerosis. Corticosteroid use (>30 mg prednisolone per day) may predispose to renal crisis.[36] Early use of ACE inhibitors, along with other improvements in managing renal crisis, has significantly reduced the mortality. Interstitial lung disease
Currently there is no consensus on the exact treatment for lung fibrosis. As stated earlier some trials have suggested benefit from the use of cyclophosphamide. Pulmonary hypertension
This is one of the most lethal complications. It can occur with established interstitial kung disease (secondary pulmonary hypertension) or without it (isolated pulmonary hypertension). The latter is associated with limited scleroderma. The use of prostacyclin analogues has been a major advance in the management of isolated pulmonary hypertension.[61] The other drugs used are warfarin and calcium channel blockers. Newer agents under trial are inhaled iloprost, nitric oxide, oral or inhaled prostacyclin formulations, and oral endothelium receptor antagonists such as bosentan.[62] Bosentan (for the pulmonary hypertension of scleroderma), cyclophosphamide (for scleroderma alveolitis) may improve organ function or functional activities, whether they are truly disease-modifying remains to be proven. Skin sclerosis
UVA1 phototherapy
Collagenase activity has been shown to be decreased in scleroderma fibroblasts[63] and UVA[1] has been tried for its collagenase inducing activity.[64] Though the exact mechanism for this is not known, singlet oxygen has been proposed as one of the factors.[65] Low dose[66],[67], medium dose[68] as well as high dose[69] UVA1 have been shown to improve skin lesions clinically as well as histopathologically in patients with localized and systemic[68] sclerosis. PUVA for scleroderma
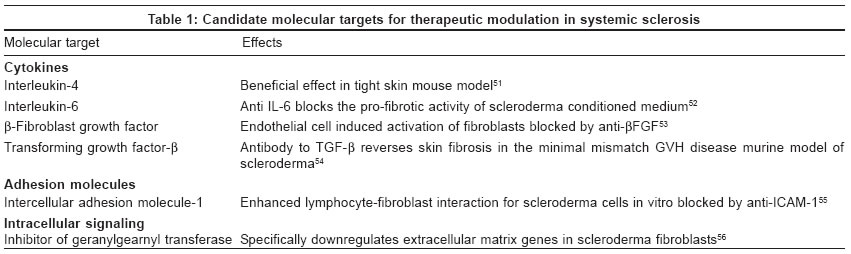
PUVA bath photochemotherapy has been tried in an effort to avoid the side effects of oral administration and found to be useful.[70],[71] Oral psoralens with UVA have been tried but with limited success.[72] Targeted molecular therapy
This has been the result of a better understanding of immunologically triggered fibrosis. Candidate molecular targets for therapeutic modulation in systemic sclerosis are listed in [Table
- 1].
SUPPORTIVE TREATMENT
Gastrointestinal reflux
Reflux can be taken care of by small frequent meals, elevating the head end of the bed, avoiding tea, coffee, alcohol and chocolate and with the use of prokinetic agents (domperidone, cisapride 10-20 mg tds,[79],[80] and mozapride 5 mg tds). Cisapride and mozapride score over domperidone because they are devoid of anti-dopamine effects. Blood levels of cisapride are increased due to inhibition of CYP3A4 by erythromycin, ketoconazole and can cause arrhythmias. Mozapride does not cause this side effect.Malabsorption
Management of secondary malabsorption requires antibiotics, such as tetracycline or doxycycline. Raynaud′s phenomenon
The number of episodes of Raynaud′s phenomenon can be decreased by warm dressing, avoiding smoking, beta blockers, methysergide, and amphetamines. Apart from calcium channel blockers and ACE inhibitors, oral 5-HT blockers,[81] local nitroglycerine paste, and sympathectomy are also useful. Arthralgias and arthritis
These can be managed by using NSAIDs, e.g. indomethacin 25 mg tds. Deformities
To prevent any deformities it is important to start physiotherapy right from the beginning. Calcinosis
Calcinosis is one of the common manifestations of scleroderma especially of the CREST syndrome. It is seen mainly in the hands around the joints and can form sterile abscesses and small ulcers that can get infected. Saline compresses can reduce the pain and swelling until the calcium is extruded. The calcium mass may be excised. Colchicine reduces the local inflamm-ation due to the calcium and promotes healing.[82] Cutaneous ulcers
Cutaneous ulcers can be protected with an occlusive dressing. Ischemic digital tip ulcers may be protected with a small plastic "cage." Adequate skin lubrication is difficult to maintain. Patients should bathe less and use moisturizers. A daily physical therapy program emphasizing a full range of motion of all large joints is important.
EXPERIMENTAL DRUGS
Recombinant human relaxin
Normally present in significant amounts in pregnant women, relaxin has been shown to reduce synthesis of type 1 collagen by scleroderma fibroblasts.[83] A dose escalating, placebo controlled trial showed benefit based on self-reported health assessment questionnaire and skin score.[84]Oral tolerization to type 1 collagen
This therapy is based on the rationale that oral tolerance to type 1 collagen can be induced, and the hypothesis that an autoimmune reaction to native collagen may contribute to the pathogenesis.[85] Oral collagen is apparently safe and may also be useful in established disease, which is otherwise difficult to treat. Anti-thymocyte globulin (ATG)
ATG is used as a treatment for scleroderma because of its efficacy as an immunosuppressive agent. There have been several encouraging case reports of the use of ATG.[86] A trial in patients with early (less than 3 years duration) diffuse scleroderma confirmed its feasibility and tolerability, but the endpoint changes were disappointing.[87] Immunoablation with autologous peripheral stem cell rescue
If scleroderma is driven by an autoimmune process, ablation of self-reactive lymphocyte clones may block pathogenesis. Pilot trials to evaluate this treatment are underway in USA.[88] Finally, here is a checklist for the treatment of systemic sclerosis:
. What every patient of systemic sclerosis should be receiving:
- Aspirin (150 mg/day)
- ACE inhibitors or angiotensin receptor blockers (enalapril 2.5-10
mg OD, losartan -25-50 mg OD)
- A calcium channel blocker can be added (nifedipine 5-20 mg tds)
- Organ specific therapy such as a proton pump blocker (omeprazole 20-40 mg OD) for esoph-ageal reflux apart from the non-pharmacological means.
. Other treatment would depend on the specific organ involvement e.g.
interstitial lung disease: cyclophosphamide.
MONITORING DISEASE ACTIVITY
- Skin thickness scores: The most widely accepted method for monitoring skin
changes in systemic sclerosis is by simple clinical palpation. The modified
Rodnan skin score employs a qualitative rating scale (0, normal skin; 1,
mild; 2, moderate; 3, severe thickening) of the findings on clinical palpation
of 17 body areas and thus is a semi-quantitative tool for clinical research
as well as a measure of clinical progress in the individual patient.[89]
- Health assessment questionnaire (HAQ)-Disability Index (DI) has been shown to be the most accurate predictor of survival; it outperformed a variety of clinical and laboratory features, including evidence of internal organ involvement in a longitudinal study of 1250 patients with 5.2 years follow up.[90] DI score correlates well with total skin thickness score, reduced fist closure, and proximal muscle weakness.[91]
- The frequency of episodes of Raynaud′s phenomenon and the
presence as well as development of new subungual ulcers are markers
of disease activity.
- Internal organ involvement and deterioration or improvement in the
same on follow up.
REFERENCES
| 1. | Hochberg MC, Silman AJ, Smolen JS, Weinblatt ME, Weisman MH. Rheumatology. 3rd ed. New York: Elsevier; 2003. Back to cited text no. 1 |
| 2. | Nimmi ME. Penicillamine and collagen metabolism. Scand J Rheumatol 1979;28:71-8. Back to cited text no. 2 |
| 3. | Harris ED, Sjoerdsma A. Effect of penicillamine on human collagen and possible application to treatment of scleroderma. Lancet 1966;2:996-9. Back to cited text no. 3 |
| 4. | Fulghum DD, Katz R. Penicillamine for scleroderma. Arch Dermatol 1968;98:51-2. Back to cited text no. 4 [PUBMED] |
| 5. | Bluestone R, Grahame R, Holloway V, Volt PJ. Treatment of scleroderma with penicillamine: a new method of observation with the effects of treatment. Ann Rheumat Dis 1970;29:153-8. Back to cited text no. 5 |
| 6. | Winkelmann RK, Kierland RR, Perry HD, Muller HD, Sams WM Jr. Management of scleroderma. Mayo Clin Proc 1971;46:128-34. Back to cited text no. 6 |
| 7. | Tio H, Van Wikk L, Haan E. Treatment of progressive systemic sclerosis with penicillamine: preliminary report of two cases. Acta Med Scand 1973;193:477-80. Back to cited text no. 7 |
| 8. | Herbert CM, Lindberg KA, Jayson MI, Bailey AJ. Biosynthesis of and maturation of skin collagen in scleroderma and effect of D-penicillamine. Lancet 1974;1:187-92. Back to cited text no. 8 [PUBMED] |
| 9. | Asboe-Hansen G. Treatment of generalized scleroderma with inhibitors of connective tissue formation. Acta Derm Venereol 1975;55:461-5. Back to cited text no. 9 [PUBMED] |
| 10. | Zachariae H, Petersen HO, Zachariae E. D-Penicillamine in scleroderma; a preliminary study. In: Munthe E, editor. Penicillamine research in rheumatoid disease. Oslo: Fabritius and Sonner; 1976. p. 290. Back to cited text no. 10 |
| 11. | Jayson MIV, Lowell C, Black CM, Wilson RS. Penicillamine therapy in systemic sclerosis. Proc R Soc Med 1977;6:92-6. Back to cited text no. 11 |
| 12. | Steen VD, Medseger TA Jr, Rodnan GP. D-Penicillamine therapy in progressive systemic sclerosis (scleroderma): a retrospective analysis. Ann Intern Med 1982;97:652-9. Back to cited text no. 12 |
| 13. | Jimenez SA, Singal SH. A 15-year prospective study of treatment of rapidly progressive systemic sclerosis with D-penicillamine. J Rheumatol 1991;18:1496-1503. Back to cited text no. 13 |
| 14. | Mellstedt H, Fagrell B, Bjokholm M. Effect on nutritional capillary circulation. Scand J Rheumatol 1977;6:92-6 Back to cited text no. 14 |
| 15. | Clements PJ, Furst DE, Wong WK, Maureen M, Barbara W, Fredrick W, et al. High dose versus low dose penicillamine in early diffuse systemic sclerosis. Arth Rheumat 1999;42:1194-1203. Back to cited text no. 15 |
| 16. | van den Hoogen FH, Boerbooms AM, Swaak AJ, Rasker JJ, van Lier HJ, van de Putte LB, et al. Comparison of methotrexate with placebo in the treatment of systemic sclerosis: a 24 week randomized double-blind trial, followed by a 24 week observational trial. Br J Rheumatol 1996;35:364-72. Back to cited text no. 16 |
| 17. | Pope JE, Bellamy N, Seibold JR, Baron M, Ellman M, Carette S, et al. A randomized controlled trial of methotrexate versus placebo in early diffuse scleroderma. Arthr Rheumat 2001;44:1351-8. Back to cited text no. 17 |
| 18. | Belch J, Ho M. Pharmacotherapy of Raynaud's phenomenon. Drugs 1996;52:682-95. Back to cited text no. 18 |
| 19. | Meyrick TRH, Rademaker M, Grimes SM, Mackay A, Kovacs IB, Cook ED, et al. Nifedipine in the treatment of Raynaud's phenomenon in patients with systemic sclerosis. Br J Dermatol 1987;117:237-41. Back to cited text no. 19 |
| 20. | Kirch W, Linder HR, Hutt HJ, Ohnhaus EE, Mahler F. Ketanserin versus nifedipine in secondary Raynaud's phenomenon. Vasa 1987;16:77-80. Back to cited text no. 20 [PUBMED] |
| 21. | Magdalena D, Christopher P, Roy S, Howell K, Blann A, Bowers E, Carol M. Losartan therapy for Raynaud's phenomenon and scleroderma. Arth Rheumat 1999;42:2646-55. Back to cited text no. 21 |
| 22. | Crawford DC, Chobanian AV, Brecher P. Angiotensin II induces fibronectin expression associated with cardiac fibrosis in the rat. Circ Res 1994;74:727-39. Back to cited text no. 22 [PUBMED] |
| 23. | Ju H, Zhao S, Jassal D, Dison JM. Effect of AT I receptor blockade on cardiac collagen remodeling after myocardial infarction. Cardiovasc Res 1997;35:223-32. Back to cited text no. 23 |
| 24. | Chua C, Diglio C, Siu B, Chua BH. Angiotensin II induces TGF- 1 in the rat heart endothelial cells. Biochem Biophys Acta 1994;1223:141-7. Back to cited text no. 24 |
| 25. | Junaid A, Rosenberg ME, Hostetter TH. Interaction of angiotensin II and TGF- in the rat remnant kidney. J Am Soc Nephrol 1997;8:1732-8. Back to cited text no. 25 [PUBMED] |
| 26. | Marshall RP, McNulty RJ, Laurent GJ. The pathogenesis of pulmonary fibrosis: Is there a fibrosis gene? Int J Biochem Cell Bio 1997;29:107-20. Back to cited text no. 26 |
| 27. | Dziado M, Denton CP, Smith R, Howell KB, Andrew B, Emma B, et al. Losartan therapy for Raynaud's phenomenon and scleroderma. Arthr Rheumat 1999;42:2646-55. Back to cited text no. 27 |
| 28. | Nishimura H, Tsuji H, Masuda H., Kasahara T, Yoshizumi M, Sugano T, et al. The effects of angiotensin metabolites on the regulation of coagulation and fibrinolysis in cultured rat aortic endothelial cells. Thromb Haemost 1999;82:1516-21. Back to cited text no. 28 |
| 29. | Vaughan DE. Fibrinolytic balance, the renin-angiotensin system and atherosclerotic disease. Eur Heart J 1998;19(Suppl G):G9-G12. Back to cited text no. 29 |
| 30. | Lopez Overjero JA, Saal SD, D'Angelo WA, Cheigh JS, Stenzel KH, Laragh JH. Reversal of vascular and renal crisis of scleroderma by oral angiotensin converting enzyme blockade. N Engl J Med 1979;300:1417-9. Back to cited text no. 30 |
| 31. | Steen VD, Constantino JP, Shapiro AP, Medseger TA Jr. Outcome of renal crisis in systemic sclerosis; relation to availability of angiotensin converting enzyme inhibitors. Ann Intern Med 1990;113:352-7. Back to cited text no. 31 |
| 32. | Steen VD, Medseger TA Jr. Severe organ involvement in systemic sclerosis with diffuse scleroderma. Arthr Rheumat 2000;43;2437-44. Back to cited text no. 32 |
| 33. | Ruddy S, Harris E, Sledge C. Scleroderma. In: Kelley's Textbook of rheumatology. 6th ed. Philadelphia: WB Saunders; 2001. p. 1229. Back to cited text no. 33 |
| 34. | Sharnoff JH, Baker LA, Shifrin A. Chronic scleroderma with acute exacerbation during corticosteroid therapy. Arch Intern Med 1951;88:783-92. Back to cited text no. 34 |
| 35. | Sharnoff JG, Carideo HL, Stein ID. Cortisone treated scleroderma. JAMA 1951;145:1230-2. Back to cited text no. 35 |
| 36. | Steen VD, Medseger TA. Case control study of corticosteroids and other agents that either precipitate or protect from the development of scleroderma renal crisis. Arthr Rheumat 1998;41:1613-9. Back to cited text no. 36 |
| 37. | Herfrich DJ, Banner B, Steen VD. Normotensive renal failure in systemic sclerosis. Arthr Rheumat 1989;32:1128. Back to cited text no. 37 |
| 38. | Pai BS, Srinivas CR, Sabitha L Efficacy of dexamethasone pulse therapy in progressive systemic sclerosis. Int J Dermatol 1995;34:726-8. Back to cited text no. 38 |
| 39. | Pasricha JS, Ramam M, Shah S. Reversal of systemic sclerosis with dexamethasone pulse. Indian J Dermatol Venereol Leprol 1990;56:43. Back to cited text no. 39 |
| 40. | Shenoi SD, Khadilkar VN, Tiwari A. Histopathological cutaneous assessment of systemic sclerosis patients after dexamethasone pulse therapy. Indian J Dermatol Venereol Leprol 2000;55:174. Back to cited text no. 40 |
| 41. | Pasricha JS, Gupta R. Pulse therapy with dexamethasone in Reiter's disease. Indian J Dermatol Venereol Leprol 1984;50:199-203. Back to cited text no. 41 |
| 42. | Schwid SR, Goodman AD, Puzas JE, McDermott MP, Mattson DH. Sporadic corticosteroid pulse and osteoporosis in multiple sclerosis. Arch Neurol 1996;53:753-7. Back to cited text no. 42 [PUBMED] |
| 43. | Lems WF, Gerrits MF, Jacobs JW, van der Brink HR, van RH, Bijlsma JW. Changes in markers of bone metabolism during high dose corticosteroid pulse treatment in patients with rheumatoid arthritis. Ann Rheum Dis 1996;55:288-93. Back to cited text no. 43 |
| 44. | Lems WF, Jacobs JW, van der Brink HR, van RH, Bijlsma JW. Transient decreases in osteocalcin and markers of type 1 collagen turnover during high dose corticosteroid pulse therapy in rheumatoid arthritis. Br J Rheumatol 1993;32:787-9. Back to cited text no. 44 |
| 45. | Silver RM, Miller KS, Kinsella MB, Smith EA, Schabel SI. Evaluation and management of scleroderma lung disease using bronchoalveolar lavage. Am J Med 1990;88:470-6. Back to cited text no. 45 [PUBMED] |
| 46. | Steen VD, Conte C, Owens GR, Medseger TA Jr. Severe restrictive lung disease in systemic sclerosis. Arthr Rheumat 1994;37:1283-9. Back to cited text no. 46 |
| 47. | Behr J, Vogelmeier C, Beinert T, Meurer M, Krombach F, Konig G, et al. Bronchoalveolar lavage for evaluation and management of scleroderma disease of the lung. Am J Respir Crit Care Med 1996;154:400-6. Back to cited text no. 47 [PUBMED] |
| 48. | White B, Moore WC, Wigley FM, Xiao HQ, Wise RA. Cyclophosphamide is associated with pulmonary function and survival benefit in patients with scleroderma and alveolitis. Ann Int Med 2000;132:947-54. Back to cited text no. 48 [PUBMED] [FULLTEXT] |
| 49. | L De Rycke, D Baeten, F Van Den Bosch, H Mielants, F de Keyser, EM Veys The effect of Infliximab on skin lesions in a patient with Scleroderma (CREST) Arthritis Res Ther 2004, 6(Suppl 1):93 Back to cited text no. 49 |
| 50. | Mayes MD, O'Donnell D, Rothfield NF, Csuka ME. Minocycline is not effective in systemic sclerosis: results of an open-label multicenter trial. Arthritis Rheum 2004;50:553-7. Back to cited text no. 50 |
| 51. | Anderegg U, Prieb J, Hildebrandt G, Saalbach A. Minocycline does not alter collagen type I metabolism of dermal fibroblasts in culture. Arch Dermatol Res 2002;294:103-8 Back to cited text no. 51 [PUBMED] [FULLTEXT] |
| 52. | Robertson LP, Marshall RW, Hickling P Treatment of cutaneous calcinosis in limited systemic sclerosis with minocycline. Ann Rheum Dis. 2003;62:267-9 Back to cited text no. 52 |
| 53. | Moreira A, Sampaio EP, Zmuidzinas A. Thalidomide exerts its inhibitory effect on TNF- by enhancing mRNA degradation. J Exp Med 1980;177:1675-80. Back to cited text no. 53 |
| 54. | Corral LG, Muller GW, Moreira AL. Selection of novel analogues of Thalidomide with enhanced tumor necrosis factor alpha activity. Mol Med 1996;2:506-15. Back to cited text no. 54 |
| 55. | Corral LG, Haslett PA, Muller GW, Chen R, Wong LM, Ocampo CJ, et al. Differential cytokine modulation and T cell activation by two distinct classes of thalidomide analogues that are potent inhibitors of TNF-alpha. J Immunol 1999;163:380-6. Back to cited text no. 55 [PUBMED] [FULLTEXT] |
| 56. | Oliver SJ, Moreira A, Kaplan G. Immune stimulation in scleroderma patients treated with thalidomide. Clin Immunol 2000;97:109-20. Back to cited text no. 56 [PUBMED] [FULLTEXT] |
| 57. | Dodman B, Rowell NR. Low molecular weight dextran in systemic sclerosis and Raynaud's phenomenon. Acta Derm Venereol 1982;62:440-2 Back to cited text no. 57 [PUBMED] |
| 58. | Wong WH, Freedman RI, Raben SF, Schwartz S, Levan NE. Low molecular weight dextran therapy for scleroderma. Effects of dextran 40 on blood flow and capillary filtration coefficient in Scleroderma. Arch Dermatol 1974;110:419-22. Back to cited text no. 58 [PUBMED] |
| 59. | Goodfield MJ, Rowell NR. Treatment of peripheral gangrene due to systemic sclerosis with intravenous pentoxifylline. Clin Exp Dermatol 1989;14:161-2 Back to cited text no. 59 [PUBMED] |
| 60. | Zachariae H, Halkier-Sorensen L, Bjerring P, Heickendorff L. Treatment of ischaemic digital ulcers and prevention of gangrene with intravenous iloprost in systemic sclerosis. Acta Derm Venereol 1996;76:236-8. Back to cited text no. 60 [PUBMED] |
| 61. | Barst RJ, Rubin LJ, Long WA, McGoon MD, Rich S, Badesch DB, et al. A comparison of continuous intravenous epoprostenol with conventional therapy for primary pulmonary hypertension. The Primary Pulmonary Hypertension Group. N Engl J Med 1996;334:296-302. Back to cited text no. 61 [PUBMED] [FULLTEXT] |
| 62. | Williamson DJ, Wallman LL, Jones R, Keogh AM, Scroope F, Penny RN, et al. Hemodynamic effects of bosentan, an endothelin receptor antagonist, in patients with pulmonary hypertension. Circ 2000;102:411-8. Back to cited text no. 62 |
| 63. | Takeda K, Hatamochi A, Ueki H. Decreased collagenase expression in cultured systemic sclerosis fibroblasts. J Invest Dermatol 1994;103:359-63. Back to cited text no. 63 |
| 64. | Scharffetter K, Wlaschek M, Hogg A. UVA irradiation induces collagenase activity in human dermal fibroblasts in vitro & in vivo. Arch Dermatol Res 1991;283:506-11. Back to cited text no. 64 |
| 65. | Wlaschek M, Briviba K, Stricklin P, Scharfetter K, Kochanek K. Singlet oxygen may mediate the UVA induced synthesis of interstitial collagenase. J of Invest Dermatol 1995;104:194-8. Back to cited text no. 65 |
| 66. | Kerscher M, Volkenandt M, Gruss C, Reuther T, von Kobyletzki G, Freitag M et al. Low dose UVA phototherapy for treatment of localized Scleroderma. J Am Acad Dermatol 1998;38:21-6. Back to cited text no. 66 [PUBMED] [FULLTEXT] |
| 67. | Kerscher M, Dirschka T, Volkenandt M . Treatment of localised scleroderma by UVA1 phototherapy. Lancet 1995;346:1166. Back to cited text no. 67 |
| 68. | Morita A, Kobayashi K, Isomura I, Tsuji T, Krutmann J. Ultraviolet A1 (340-400 nm) phototherapy for scleroderma in systemic sclerosis. J Am Acad Dermatol 2000;43:670-4. Back to cited text no. 68 [PUBMED] [FULLTEXT] |
| 69. | Stege H, Berneburg M, Humke S, Klammer M, Grewe M, Grether-Beck S et al. High-dose UVA1 radiation therapy for localized Scleroderma. J Am Acad Dermatol 1997;36(6 Pt 1):938-44. Back to cited text no. 69 |
| 70. | Kerscher M, Volkenandt M, Meurer M, Lehmann P, Plewig G, Rocken M. Treatment of localised scleroderma with PUVA bath photochemotherapy. Lancet 1994;343:1233. Back to cited text no. 70 |
| 71. | Morita A, Sakakibara S, Sakakibara N, Yamauchi R, Tsuji T. Successful treatment of systemic sclerosis with topical PUVA. J Rheumatol 1995;22:2361-5. Back to cited text no. 71 [PUBMED] |
| 72. | Hofer A, Soyer HP. Oral psoralen-UV-A for systemic Scleroderma. Arch Dermatol 1999;135:603-4. Back to cited text no. 72 [PUBMED] [FULLTEXT] |
| 73. | Ong C, Wong C, Roberts CR, The HS, Jirik FR. Anti-IL-4 treatment prevents dermal collagen deposition in the tight skin mouse model of scleroderma. Eur J Immunol 1998;28:2619-29. Back to cited text no. 73 |
| 74. | Feghali CA, Boulware DW, Levy LS. Mechanisms of pathogenesis in scleroderma. Effects of serum and conditioned culture medium on fibroblast function in scleroderma. J Rheumat 1992;19:1212-19. Back to cited text no. 74 |
| 75. | Denton CP, Xu S, Black CM, Pearson JD. Scleroderma fibroblasts show increased responsiveness to endothelial cell derived IL-1 and beta-FGF. J Inv Dermat 1997;108:269-74. Back to cited text no. 75 |
| 76. | McCormick LL, Zhang Y, Tootell E, Gilliam AC. Anti-TGF-beta treatment prevents skin and lung fibrosis in murine sclerodermatous GVH disease; a model of human scleroderma. J Immunol 1999;163:5693-9. Back to cited text no. 76 [PUBMED] [FULLTEXT] |
| 77. | Abraham D, Lupoli S, McWhirter A. Expression and function of surface antigens on scleroderma fibroblasts. Arthr Rheumat 1991;34:1164-72. Back to cited text no. 77 |
| 78. | Rosenbloom J, Saitta B, Gaidarova S, Sandorfi N, Rosenbloom JC, Abrams WR, et al. Inhibition of type 1 collagen gene expression in normal and systemic sclerosis fibroblasts by a specific inhibitor of geranylgeranyl transferase 1. Arthr Rheumat 2000;43:1624-1632. Back to cited text no. 78 |
| 79. | Horowitz M, Maddern GH, Maddox A, Wishart J, Chatterton BE. Effects of cisapride on gastric and esophageal emptying in progressive systemic sclerosis. Gatsroenterology 1987;93:311-5. Back to cited text no. 79 |
| 80. | DeVault KR, Castell DO. Current diagnosis and treatment of gastroesophageal reflux disease. Mayo Clin Proc 1994;69:867-76. Back to cited text no. 80 [PUBMED] |
| 81. | Seymoens J. Ketanserin: a novel cardiovascular drug. Blood Coagul Fibrinolysis 1990;1:219-24. Back to cited text no. 81 |
| 82. | Fuchs D, Fruchter L, Fishel B, Holtzman M, Yaron M. Colchicine suppression of local inflammation due to calcinosis in dermatomyositis and progressive systemic sclerosis. Clin Rheum 1986;5:527-30. Back to cited text no. 82 |
| 83. | Unemori EN, Pickford LB, Salles AL, Piercy CE, Grove BH, Erickson ME, et al. Relaxin induces an extracellular matrix degrading phenotype in human lung fibroblasts in vitro and inhibits lung fibrosis in a murine model in vivo. J Clin Inv 1996;98:2739-45. Back to cited text no. 83 |
| 84. | Seibold JR, Korn JH, Simms R, Clements PJ, Moreland LW, Mayes DM, et al. Recombinant human relaxin in the treatment of scleroderma. A randomized, double blind, placebo controlled trial. Ann Int Med 2000;132:871-9. Back to cited text no. 84 |
| 85. | McKown KM, Carbone LD, Bustillo J, Seyer JM, Kang AH, Postlethwaite AE. Induction of immune tolerance to human type 1 collagen in patients with systemic sclerosis by oral administration of bovine type 1 collagen. Arthr Rheumat 2000;43:1054-61. Back to cited text no. 85 |
| 86. | Tarkowski A, Anderson-Gare B, Aurell M. Use of anti-thymocyte globulin in the management of refractory systemic autoimmune diseases. Scand J Rheumat 1993;22:261-6. Back to cited text no. 86 |
| 87. | Matterson EL, Sheeb MI, McCarthy TG, Calamia KT, Mertz LE, Goronzy JJ. Pilot study of antithymocyte globulin in systemic sclerosis. Arthr Rheumat 1996;39:1132-7. Back to cited text no. 87 |
| 88. | Clements PJ, Furst DE. Choosing appropriate patients for autologous stem cell transplantation. J Rheumat Supplement 1997;48:85-8. Back to cited text no. 88 |
| 89. | Clements PJ, Lachenbruch P, Seibold J. Inter- and intraobserver variability of total skin thickness score (modified Rodnan TSS) in systemic sclerosis. J Rheumatol 1995;22:1281. Back to cited text no. 89 |
| 90. | Steen VD, Medsger TA Jr. The value of the Health Assessment Questionnaire and special patient-generated scales to demonstrate change in systemic sclerosis patients over time. Arthr Rheumat 1997;40:1984-91. Back to cited text no. 90 |
| 91. | Clements PJ, Wong WK, Hurwitz EL, Furst DE, Daniel EM, Maureen WB, et al. Correlates of disability index of the health assessment questionnaire. Arthr Rheumat 1999;42:2372-80. Back to cited text no. 91 |
Copyright 2004 - Indian Journal of Dermatology, Venereology, Leprology
The following images related to this document are available:
Photo images
[dv04022t1.jpg]
[dv04022f2.jpg]
[dv04022f1.jpg]
|

{kind=link}
{kind=link}
{kind=link}