 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
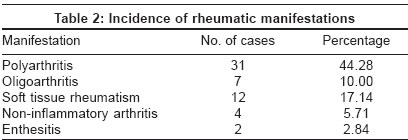
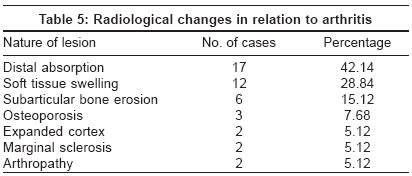
Indian Journal of Dermatology, Venereology, Leprology, Vol. 70, No. 2, March-April, 2004, pp. 76-78 Studies A study of rheumatological manifestations of leprosy Vengadakrishnan K, Saraswat PradeepK, Mathur PC Department of Medicine, G. R. Medical College and J. A. Group of Hospitals, Gwalior Code Number: dv04023 ABSTRACT BACKGROUND AND AIMS: Rheumatic manifestations are a common feature of leprosy. The present study was performed to assess the incidence of rheumatic manifestations in leprosy. METHODS: Seventy cases of leprosy attending the indoor and outdoor departments were studied. RESULTS: Out of the 70 cases studied, rheumatic manifestations were seen in 61.42% of cases: arthritis in 54.28% and soft tissue rheumatism in 17.14%. Enthesitis was seen in 2.84% of cases. The incidence of arthritis in lepra reactions was 57.57%. CONCLUSIONS: Musculoskeletal manifestations can occur at any time during the infection. Articular inflammation in leprosy usually occurs in reactive states, particularly erythema nodosum leprosum (ENL). Leprosy can present with arthritis as the first symptom.INTRODUCTION Leprosy can present with a variety of clinical manifestations. Musculoskeletal symptoms are the third most common manifestation (after dermatological and neurological involvement) of the disease. Rheumatic manifestations may be the primary complaint, delaying accurate diagnosis. A plethora of rheumatic manifestations are associated with leprosy, particularly with lepra reactions.[1] The rheumatological manifestations of leprosy occur singly or in varying combinations, particularly in reactional states.[2],[3],[4] Arthritis in leprosy closely mimics other rheumatic disorders.[5] Enthesitis (tenderness to palpation at the site of attachment of bone to tendon, ligament or joint capsule) has been reported as a manifestation of leprosy.[6],[7] Rheumatoid factor, C-reactive protein, antistreptolysin O antibody, antinuclear antibody (ANA) and antineutrophil cytoplasmic antibody (ANCA) have been reported with varying incidences in different forms of leprosy.[8],[9],[10],[11] The osteoarticular changes in leprosy are considered to be a consequence of specific or nonspecific injuries.[12],[13] The aims of this study were to determine the incidence of rheumatic manifestations in histologically proven cases of leprosy, the incidence of arthritis in lepra reactions and the incidence of positive rheumatic markers and radiological changes in cases of arthritis in leprosy. METHODS The present study included 70 patients of leprosy attending the Skin & V. D. OPD and wards, and Leprosy Clinic. All of them were clinically examined, investigated and classified. Skin and nasal smears were obtained and examined for AFB by the Ziehl-Neelson staining method. The bacteriological and the morphological indices were calculated. A skin biopsy was taken from lesions typical of leprosy and histopathological findings were noted. A complete hemogram, urine routine examination, serum bilirubin, renal profile, blood sugar, serological markers (such as rheumatoid factor, ASO titer and C-reactive protein) and radiology of the affected parts was done in all cases. RESULTS Seventy histologically proven patients of leprosy were included: 27 cases of borderline leprosy, 16 of tuberculoid leprosy, 15 of lepromatous leprosy and 12 of indeterminate leprosy. Forty-three (61.42%) of them were males. The age distribution of patients is shown in [Table - 1]. Common clinical signs were thickened nerves (82%), anesthetic patch (54%) and arthritis (54.28%). Two patients had gangrene, while four had a trophic ulcer. Forty-three patients had rheumatic manifestations (61.42%), with arthritis predominating (38 patients) [Table - 2]. The manifestations were most commonly seen in patients with borderline lepromatous leprosy (27%), followed by those with tuberculoid leprosy (13%). Most patients had symmetric peripheral polyarthritis (54%), most commonly involving the knee, elbow, and the metacarpophalangeal and interphalangeal joints of the hands. Most patients had a symmetric peripheral polyarthritis of the small joints of the hands and feet clinically indistinguishable from rheumatoid arthritis. In contrast to rheumatoid arthritis, males had a greater incidence of leprous arthritis (34% in males and 20% in females). None of the patients had subcutaneous nodules or other extra-articular manifestations of rheumatic disorders. C-reactive protein was positive in 39 cases (55.71%), mostly in lepromatous leprosy patients (66.66%). It was more commonly found in patients with arthritis (42.1%) than in those without arthritis (15.61%). Rheumatoid factor was positive in 24 cases (34.9%) [Table - 3] and [Table - 4], more commonly in lepromatous leprosy patients (60%). It was positive in 21% of patients with arthritis and 15.61% without arthritis (out of 38 cases). ASO was positive in about 51.42% (36 cases). All patients with arthritis (38 cases) were subjected to X-ray of the concerned joints. Non-specific changes were found commonly (33 cases; 86.84%) [Table - 5]. Lepra reactions, usually type 1 (31 cases; 93%), were found in 33 cases (47%), generally in patients with borderline leprosy. The incidence of arthritis in lepra reactions was 57%. The wrist joint was involved in 94.73%. The other commonly involved joints were the knee, elbow, metacarpophalangeal and interphalangeal joints. DISCUSSION Symmetric polyarthritis involving the peripheral joints is the most common rheumatic manifestation in leprosy patients. Our study included a random group of patients with leprosy ranging from mild disease to severe deformity in contrast to other studies which have examined a representative sample of patients.[3],[4],[6],[7] Nonetheless the incidence of arthritis was consistent with the findings of previous studies. Because of similarities in the presentation of arthritis and the joints involved, leprous arthritis simulates rheumatoid arthritis. The absence of nodules or extra-articular manifestations, males being more commonly affected than females, and response to anti-leprosy treatment were the clinical distinguishing features in our study and other studies.[1],[2],[5] The histopathological changes differentiate leprous arthritis from rheumatic disorders. We could not establish or rule out a combination of leprosy and a rheumatic disorder because investigations like ANA, ANCA and specific rheumatic markers were not done because the patients could not afford them.[10],[11] Rheumatic markers had increased positive values in our study. The ASO antibody was commonly seen in patients of leprosy. Due to the common occurrence of false positive reactions, the exact incidence of serological markers could not be established. Earlier studies have also found an increased incidence but have not clearly established their association with arthritis.[7],[8],[9] Nonspecific bone changes were common and this has been noted by other authors too.[12],[13] Our study shows that arthritis is common in leprosy and involves the peripheral joints most commonly. Early recognition of leprosy in a patient presenting with rheumatic manifestations is important for proper treatment and prevents further deformity. REFERENCES
Copyright 2004 - Indian Journal of Dermatology, Venereology, Leprology The following images related to this document are available:Photo images[dv04023t3.jpg] [dv04023t2.jpg] [dv04023t5.jpg] [dv04023t1.jpg] [dv04023t4.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}