 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
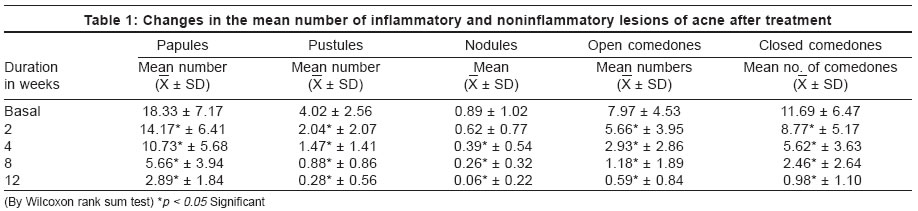
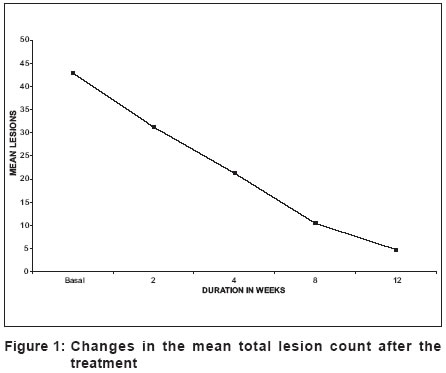
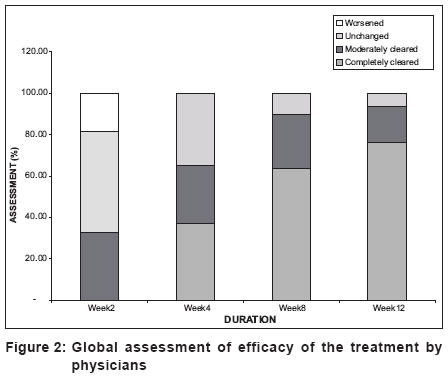
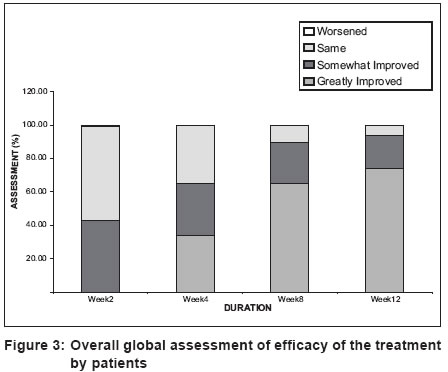
Indian Journal of Dermatology, Venereology, Leprology, Vol. 70, No. 2, March-April, 2004, pp. 92-95 Studies An open study to evaluate the efficacy and safety of tazarotene gel (0.1%) in acne vulgaris Saple DG, Torsekar RG, Pawanarkar Vikas , Dhanalakshmi UR, Ravichandran G, Kaur Daljeet , Dongre Neelesh , Desai Anish Glenmark Pharmaceuticals Ltd, Mumbai Code Number: dv04027 ABSTRACT BACKGROUND: Tazarotene is a new third generation topical acetylenic retinoid. The present study was conducted to evaluate the efficacy and safety of tazarotene gel (0.1%) in Indian patients of acne vulgaris. METHODS: The present study was a prospective, open, multicentric, phase III trial. The duration of study was 14 weeks, including a 12-week active treatment period, preceded by a 2-week washout phase. Patients applied 0.1% tazarotene gel as a thin film over the affected area once daily in the evening. The efficacy was evaluated by analyzing changes in the number of facial acne lesions and patient's and physicians' global assessment. The efficacy parameters were assessed at baseline, visits 2, 4, 8, and 12 weeks. Tolerability and safety was assessed by physical examination, laboratory parameters and evaluation of adverse events. RESULTS: A total of 126 patients in 6 centers completed the study. At the end of the 8th and 12th weeks, the mean number of inflammatory lesions reduced by 70.6% and 86.1%, non-inflammatory lesions by 81.5% and 92%, and total lesion count 75.6% and 88.8% respectively from baseline. Also, 90.7% and 93.6% of total study cases showed complete to moderate clearance of acne lesions according to physicians at the end of the 8th and 12th weeks. CONCLUSIONS: This study confirms the efficacy and safety of tazarotene gel (0.1%) in Indian patients of acne vulgaris.INTRODUCTION Acne vulgaris is one of the most common disorders treated by dermatologists. Obstruction of the sebaceous follicle is the principal pathologic event, with formation of a microcomedo, the precursor of all acne lesions. When this obstruction occurs, the continued production of sebum and keratin gives rise to visible non-inflammatory lesions, open comedones (blackheads) and closed comedones (whiteheads). Leakage or rupture of the contents of the comedones into the dermis causes inflammatory acne.[1] The use of many of the available topical therapies is limited by inadequate long term efficacy, adverse effects and/or lack of cosmetic acceptability. Tazarotene is a new third generation topical acetylenic retinoid. It normalizes keratinocyte differentiation, reduces keratinocyte proliferation and decreases expression of inflammatory markers. The selectivity of tazarotene for the beta and gamma subtypes of retinoic acid receptors minimizes the risk of adverse effects. Tazarotene has a low potential for systemic adverse effects due to minimal absorption, its rapid metabolism into hydrophilic metabolites and rapid elimination from the body. There is no systemic accumulation of the drug. Once-daily application leads to better patient compliance. Tazarotene was approved by the US-FDA in June 1997 for acne vulgaris.[2] The present study evaluated the efficacy and safety of tazarotene gel (0.1%) in Indian patients of acne vulgaris. METHODS The present study was a prospective, multicentric, open-label, phase III study conducted in 6 centers. All patients or their guardians provided written informed consent before screening and enrollment in the study. The trial was conducted in accordance with the principles of Good Clinical Practice and the Declaration of Helsinki. The study protocol was approved by the concerned Institutional Review Board. Patients of both sexes in the age group of 13-30 yrs with the clinical diagnosis of acne vulgaris and having comedones, papules, pustules (£ 5), or nodules (£ 2) were enrolled in the study. Exclusion criteria were pregnancy and lactation; known hypersensitivity to the drug; severe acne (acne fulminans, acne conglobata, etc.); and severe skin, hepatic, renal or systemic diseases. The duration of the study was 14 weeks, consisting of a 2-week washout phase followed by a 12-week active treatment period. Patients applied 0.1% tazarotene gel as a thin film over the affected area once daily in the evening. The efficacy was evaluated by analyzing changes in the number of facial acne lesions, i.e. total lesion count (inflammatory + noninflammatory lesions), inflammatory lesion count (papules, pustules, nodules), and non-inflammatory lesion count (open and closed comedones), and patient′s and physician′s global evaluation. These efficacy parameters were assessed at baseline, and at visits at 2, 4, 8, and 12 weeks. The general clinical safety was monitored by the incidence of treatment-emergent adverse events, physical examination, and changes in clinical laboratory variables. Adverse events were monitored at baseline and throughout the study. The statistical analysis was done using the Wilcoxon rank sum test. A p value < 0.05 was considered significant. RESULTS A total of 136 patients in 6 centers were included in the study; 126 patients successfully completed it. The ten patients lost to follow up were not included in the final analysis. [Table - 1] shows the changes in the inflammatory and non-inflammatory lesions of acne. A statistically significant fall was seen by 8 and 12 weeks in the mean number of papules (69.1% and 84.2% respectively), pustules (78.1% and 93% respectively), nodules (70.8% and 93.3% respectively), open comedones (85.2% and 92.6% respectively), and closed comedones (79% and 91.6% respectively). The mean inflammatory acne lesions reduced from 23.25 at baseline by 70.6% and 86.1% at the end of the 8th week and 12th week respectively, which was statistically significant. The non-inflammatory acne lesions fell from 19.67 at baseline by 81.5% and 92% at the end of the 8th week and 12th week respectively; this too was statistically significant. The mean total lesion count reduced from 42.94 at baseline by 75.6% and 88.8% at the end of the 8th week and 12th week respectively, which was statistically significant [Figure - 1]. At the end of the 8th week and the 12th week, 90.7% and 93.6% respectively of total study cases showed complete to moderate clearance of acne lesions according to physicians [Figure - 2]. According to the global evaluation of efficacy by patients, at the end of the 8th week and the 12th week, 89.7% and 93.6% of total study cases respectively showed great to somewhat improvement in acne lesions [Figure - 3]. Untoward effects were experienced by 11.9% of patients during the treatment, most commonly itching (4.8%), erythema (2.4%) and dryness, and burning (1.6%). DISCUSSION There was a statistically significant improvement in the inflammatory and non-inflammatory lesions of acne. The beneficial effects were seen as early as two weeks of treatment. According to the physician′s evaluation at the end of treatment, 93.6% of patients showed almost complete clearance of acne lesions. Once daily application led to good patient compliance. These findings confirm the efficacy of the drug in the Indian population. The basis of tazarotene′s therapeutic effect in acne may be in its anti-hyperproliferative, normalizing of differentiation and anti-inflammatory effects.[3] Tazarotene inhibited corneocyte accumulation in rhino mouse skin and cross-linked envelope formation in cultured human keratinocytes. After topical application percutaneous penetration is limited, with less than 6% of the applied drug being absorbed into the bloodstream.[4] Tazarotene is rapidly metabolized into tazarotenic acid and other metabolites that are not lipophilic. Tazarotene and its metabolites are rapidly eliminated from the blood in the urine and feces. Hence there is no systemic accumulation of the drug. It does not show tachyphylaxis.[5] The efficacy of tazarotene in acne is well established in studies conducted in the US.[6],[7] It can also be used as short contact therapy where application, after an initial contact period of 2 minutes, is increased in 1-minute increments, at intervals of at least 3 days, to a maximum of 5 minutes. The contact period is reduced to 30 seconds if there is peeling, erythema, dryness, burning, or itching; the contact period is then increased in 30-second intervals every 3 days, if tolerated, to a maximum of 5 minutes.[8] Tazarotene (0.1%) was found to be superior to adapalene (0.1% gel) and tretinoin (0.025%, 0.1%) for the treatment of acne vulgaris.[7],[9],[10],[11] Clinical studies have confirmed the safety profile of tazarotene.[12] In our study 11.9% of the patients had side effects due to treatment, mainly itching (4.8%), erythema and dryness (2.4%), and burning (1.6%). These were mild in nature and decreased with the continuation of therapy. There was no report of any serious adverse event. The drug was very well tolerated. There were no study dropouts because of adverse events. However, 10 patients were lost to follow up and were not included in the final analysis. No significant laboratory changes could be detected, which indicates a good laboratory safety profile. In conclusion, this study confirms the efficacy, safety and tolerability of tazarotene gel (0.1%) in Indian patients of acne vulgaris. REFERENCES
Copyright 2004 - Indian Journal of Dermatology, Venereology, Leprology The following images related to this document are available:Photo images[dv04027f1.jpg] [dv04027t1.jpg] [dv04027f3.jpg] [dv04027f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}