 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Dermatology, Venereology, Leprology, Vol. 70, No. 2, March-April, 2004, pp. 96-98 Studies Progressive systemic sclerosis in childhood: A report of three cases Belgaumkar Vasudha Abhijit , Gokhale Neeta R, Mahajan Pradeep M, Tolat Sunil N, Bhokare Anil , Kamble Shekhar Department of Dermatology, Venereology and Leprosy,
B. J. Medical College and Sassoon General Hospitals, Pune - 411 01 Code Number: dv04028 ABSTRACT Systemic sclerosis is unusual in childhood. We describe three children who presented with diffuse hidebound skin associated with gastrointestinal and pulmonary abnormalities. Cardiac and renal dysfunctions, which are often encountered in these patients, were notably absent in our cases.INTRODUCTION Scleroderma in childhood ranges from circumscribed and self-limited disease to diffuse skin involvement and multiple internal organ derangements with fatal outcome. Compared to adults, progressive systemic sclerosis is rare in young persons.[1] Only 1.5% of all cases occur under the age of 10 years, with females constituting at least two-thirds of the cases.[2] Here we present three children with sclerosis of the skin and associated pulmonary and gastrointestinal involvement. CASE
REPORT
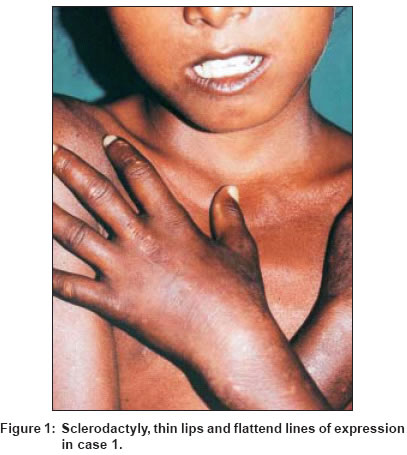
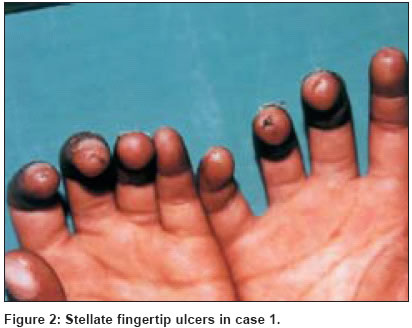
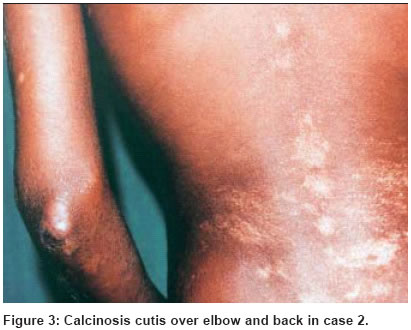
Case 1 On examination, the hands, forearms and trunk showed hidebound skin. The face revealed a pinched nose and microstomia with a positive Ingram′s sign. Other findings were sclerodactyly with a positive Raynaud′s phenomenon, stellate ulcers over the fingertips, and salt and pepper appearance of the skin over the forehead, extremities and back [Figure - 1] and [Figure - 2]. On investigation, anemia and raised ESR were detected. An X-ray of the chest was normal while that of the hands showed reduced periarticular bone density. Pulmonary function tests showed decreased vital capacity with restrictive lung disease. Barium studies revealed hampered peristalsis of the esophagus suggestive of dysmotility. The ANA, RA factor, VDRL and LE cell tests were normal. The skin biopsy was suggestive of scleroderma. Case 2 His pulmonary function tests were suggestive of a restrictive pattern with decreased FEV1 and vital capacity. Barium studies revealed sluggish peristalsis with dilated esophagus. The ANA, VDRL, RA factor and LE cell tests were negative. The skin biopsy showed collagenization of the dermis with high placed eccrine glands. Case 3 DISCUSSION Although resembling adult progressive systemic sclerosis (PSS), juvenile onset disease has a number of distinguishing features.[3],[4] Similar to adult disease, it is characterized by Raynaud′s phenomenon (90-95%), diffuse skin involvement and a microvasculopathy leading to progressive dysfunction of the esophagus, lungs, heart and kidney. All three patients presented with typical cutaneous features with two cases showing calcinosis cutis. Pulmonary involvement, though invariable in PSS, may remain asymptomatic or may present with dyspnea and cough. Although our patients were asymptomatic, they all showed a restrictive type of lung disease on pulmonary function tests. Esophageal dysfunction occurs in most patients, although only half will complain of dysphagia.[2] One of our patients had dysphagia while barium studies revealed esophageal involvement in two patients. Bodemer et al have reported that cardiac abnormalities like pericarditis, left or biventricular failure or arrhythmias are common in pediatric systemic sclerosis.[5] Only one of our patients showed tachycardia with right ventricular dominance secondary to pulmonary involvement. Renal involvement is seen in 40-60% patients in the form of malignant hypertension, proteinuria, and azotemia. It generally occurs rapidly within the first three years of PSS and indicates a guarded prognosis.[2] None of our 3 patients have so far developed any clinical or laboratory abnormalities suggestive of renal dysfunction. Antinuclear antibodies are reported in 70% to 90% of patients. Only one of our 3 patients showed ANA positivity. All three patients and their families were counseled regarding the slow progression of this disorder and supportive measures like protection from the cold, etc. As the beneficial effect of D-penicillamine is greater if it is started within the first three years, and considering the systemic involvement, it was started in all three patients in a dose of 3 mg/kg per day along with nifedipine. This dose can be increased every month up to a maximum of 10-15 mg/kg per day according to the response and tolerance to therapy. The prognosis in childhood scleroderma depends on functional impairment and the course of visceral disease is difficult to predict.[6] However, Foeldvari et al have reported that most patients of juvenile systemic sclerosis show a favorable outcome and a significantly better survival rate as compared to their adult counterparts.[7] Thus the prefix ′progressive′ is not uniformly applicable and should be avoided. REFERENCES
Copyright 2004 - Indian Journal of Dermatology, Venereology, Leprology The following images related to this document are available:Photo images[dv04028f2.jpg] [dv04028f1.jpg] [dv04028f3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}