 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
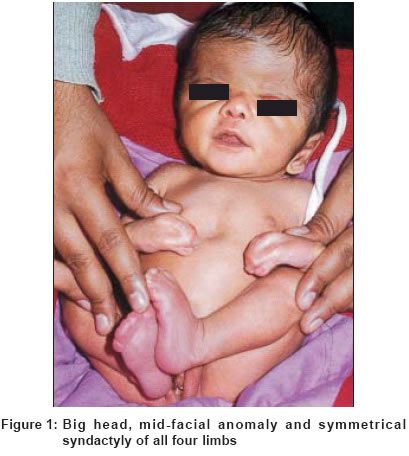
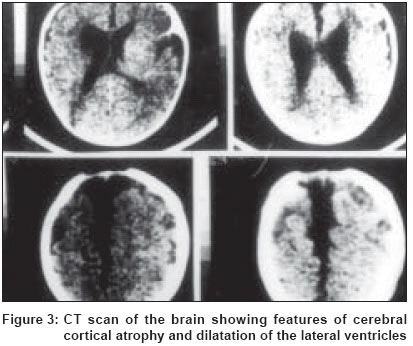
Indian Journal of Dermatology, Venereology, Leprology, Vol. 70, No. 2, March-April, 2004, pp. 105-107 Case Report Apert's syndrome Mukhopadhyay Amiya Kumar , Mukherjee Debjani Consultant Dermatologist, Asansol, WB Code Number: dv04031 ABSTRACT Apert's syndrome (acrocephalosyndactyly) is a rare congenital disorder characterized by craniosynostosis, mid-facial malformations and symmetrical syndactyly. We present a 2-month-old girl having features of Apert's syndrome, with cerebral cortical atrophy and bifurcation of the right first metatarsal base, a hitherto undescribed finding. INTRODUCTION Apert′s syndrome, also known as acrocephalosyndactyly, is a rare congenital disorder first described in 1906. It is characterized by craniosynostosis, mid-facial malformations and symmetrical syndactyly.[1] Mental retardation is common, but not invariable, and its severity may not be marked. These patients may have frontal bossing, a narrow palate, and broad, short and fused nails with micronychia.[2] Apert′s syndrome has been rarely reported in India.[3] We present a patient of Apert′s syndrome who has cerebral cortical atrophy and bony abnormalities of the right foot. CASE REPORT A 2-month-old girl, delivered by Caesarian section (due to a big head) four weeks prior to the due date of delivery, presented with multiple congenital anomalies, which included a large head with frontal bossing and syndactyly of all four limbs. Her parents were in their mid twenties and there was no history of consanguinuity. The mother′s pregnancy was uneventful, with no history of any disease, medication and addiction during that period. Clinical examination suggested that the patient′s metopic suture and posterior fontanelle were open, but the coronal suture was closed. She had a depressed bridge of the nose, upward slanting of the eyes, small multiple acneiform lesions on the nose, a low posterior hairline and a narrowed high arched palate. The patient also had a small epigastric hernia. Examination of the upper limbs showed syndactyly of all digits, out of which the second, third and fourth ones were more fused, almost forming a single unit with a single, small and broad nail. The lower limbs also showed symmetrical syndactyly leading to the fusion of all toes [Figure - 1]. Systemic examination revealed no abnormality. Radiological examination of the skull showed that the vault was large in size, with increased antero-posterior and transverse diameter. Thinning of the outer table was noted with marked enlargement of the fontanelle. Hypertelorism of the orbits was seen. The sella was normal in dimension and shape. An X-ray of both hands showed syndactyly with webbing of the skin. The 4th and 5th metacarpals were fused and the distal phalanges malformed. An X-ray of the feet also revealed syndactyly, but the metatarsals showed no fusion. Abnormal position of the phalanges of the 1st and 2nd toes was found. The right first metatarsal showed bifurcation at the base [Figure - 2]. A Plain CT scan of the brain showed hydrocephalus with prominent cisterna magna and dilated lateral ventricles. Atrophy of the frontal and parietal lobes was noted [Figure - 1]. Gray and white matter discriminability was good. There was no abnormal calcification. DISCUSSION Apert′s syndrome is an autosomal dominant disorder but in many cases the inheritance is sporadic.[4] An association between this condition and a high parental age has been suggested.[5] A localized mutation of the gene for Fibroblast growth factor 2 (FGFR2) with chromosomal localization at 10q26 is responsible for this disorder.[1] Apert′s syndrome is thought to occur as a result of androgen end organ hyper-response affecting the epiphyses and sebaceous glands.[6] This results in early epiphyseal fusion resulting in short stature, short and fused digits and acrocephaly. Patients of Apert′s syndrome often have acne that is severe, extensive and resistant to treatment. In one series, seven of nine patients developed moderate to severe acne at puberty and had lesions on the arms and forearms in addition to the commonly affected sites.[7] The defect of FGFR2 which is found in Apert′s syndrome is also recorded in the acneform lesions in Munro nevus.[8] The skin, eyes and hair may show pigmentary dilution.[9] Other cutaneous abnormalities reported are hyperhidrosis[10] and oculocutaneous albinism.[1] Cerebral cortical atrophy with dilation of the lateral ventricle as in our patient may lead to mental subnormality. The bifurcation of the right first metatarsal base seen in this patient is a bony abnormality that has not been described earlier in Apert′s syndrome. Another case of thickened first metacarpal forked at the base has been reported.[3] As already mentioned, androgen hyper-response of the epiphysis leads to fusion of the bones, but whether any such factor is responsible for the bifurcation of the base of the metatarsals/metacarpals is not known. REFERENCES
Copyright 2004 - Indian Journal of Dermatology, Venereology, Leprology The following images related to this document are available:Photo images[dv04031f2.jpg] [dv04031f3.jpg] [dv04031f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}