 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
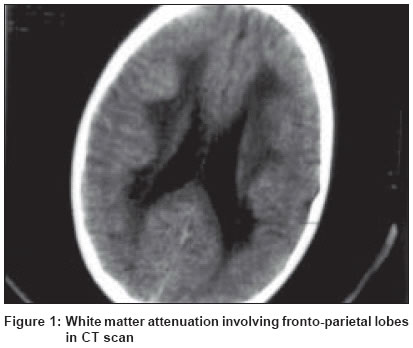
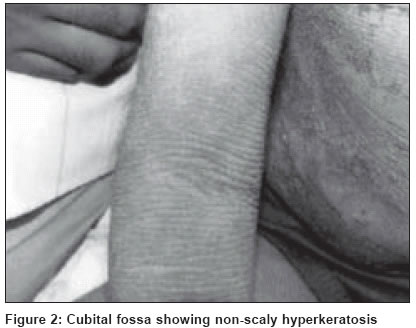
Indian Journal of Dermatology, Venereology, Leprology, Vol. 70, No. 2, March-April, 2004, pp. 110-111 Case Report Sjogren-Larsson syndrome: Report of two cases Uppal Monica , Srinivas CR, Thowfeeq KT Department of Dermatology, PSG Institute of Medical Sciences & Research, Coimbatore Code Number: dv04033 ABSTRACT Two cases of Sjogren-Larsson syndrome are discussed along with a review of the literature. Both the patients had generalized ichthyosis, spastic paraplegia, mental retardation and ophthalmologic examination showing glistening foveal and parafoveal dots.INTRODUCTION Sjogren-Larsson syndrome (SLS) is a rare autosomal recessive disorder. It was first reported in 1957 by Sjogren and Larsson, two Swedish doctors.[1] It is characterized by the triad of ichthyosis, mental retardation and spastic diplegia or quadriplegia.[2],[3],[4] Other common features include short stature, kyphoscoliosis and retinal changes.[4] We report two cases with typical features of Sjogren-Larsson syndrome. CASE REPORT Case 1A 10-year-old girl presented with ichthyosis and spastic paraplegia since infancy. She had erythema at birth, and subsequently scaling was noticed on the abdomen, back, extremities, axillae and cubital fossae. She had delayed speech development. Examination revealed mental retardation, kyphotic deformity of the spine and spastic paraplegia with ankle clonus. Lamellar ichthyosis was present on the extensors of both legs. Both cubital fossae and axillae showed accentuated skin markings. The face, palms, soles, nails and teeth appeared normal. Ophthalmological examination revealed the presence of foveal and parafoveal glistening dots. A CT scan of the brain showed diffuse white matter attenuation involving the fronto-parietal lobes predominantly, evident as white matter hypodensity [Figure - 1]. A biopsy from the volar aspect of the forearm showed orthohyperkeratosis, acanthosis and a sparse perivascular chronic inflammatory infiltrate in the dermis. Case 2 Examination revealed mental retardation and spastic paraplegia with ankle clonus. Cutaneous examination showed lamellar ichthyosis of both legs and non-scaly hyperkeratotic thickening of the skin in the neck, axillae and cubital fossae [Figure - 2]. The scalp showed furfuraceous scales. Mild palmoplantar thickening was present. The nails, teeth and oral mucosa were normal. Ophthalmologic examination showed parafoveal glistening dots consistent with the diagnosis of SLS. Biopsy and CT scan were not done. DISCUSSION The cutaneous and central nervous system manifestations of SLS are attributed to a defect in the metabolism of long chain fatty acids. There is deficiency of the fatty aldehyde dehydrogenase (FALDH) component of the fatty alcohol oxidoreductase (FAO) complex due to a recessive mutation of the FALDH gene located on the short arm of chromosome 17 (17p11.2).[1],[5] This results in the accumulation of fatty alcohols in the skin and myelin of the central nervous system. The ichthyosis of SLS is characteristically of three types: furfuraceous, lamellar or non-scaly hyperkeratotic thickening of the stratum corneum.[6] Lamellar ichthyosis is present on the legs. The non-scaly hyperkeratosis produces a characteristic accentuation of the skin markings in the flexures. The hair, nails and teeth are unaffected. The occurrence of glistening dots on fundus examination strongly suggests SLS.[6] Histopathology shows orthohyperkeratosis, acanthosis and papillomatosis. The granular cell layer is normal or increased with a mild upper dermal inflammatory change. Measurement of FALDH enzyme activity in cultured fibroblasts and leukocytes is a specific marker and reliable biochemical diagnostic test for SLS.[1] Ichthyosis is responsive to treatment with emollients, keratolytics and retinoids. Intensive physiotherapy improves motor and social development in SLS. Orthopedic treatment of skeletal deformities may help some cases. Therapeutic trials of zileuton, a 5-lipoxygenase inhibitor, have been shown to decrease the pain and pruritus associated with SLS.[7] REFERENCES
Copyright 2004 - Indian Journal of Dermatology, Venereology, Leprology The following images related to this document are available:Photo images[dv04033f1.jpg] [dv04033f2.jpg] |
| |||||||||

{kind=link}
{kind=link}