 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
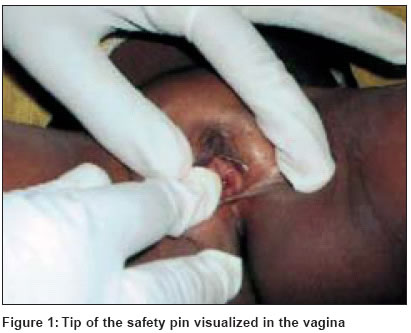
Indian Journal of Dermatology, Venereology, Leprology, Vol. 70, No. 2, March-April, 2004, pp. 118-119 Letter To Editor Foreign body in the vagina of a 3½-year-old child: Sexual abuse or a childish prank? Padmavathy L, Ethirajan N, Rao LLakshmana Departments of Community Medicine, Rajah Muthiah Medical College, Annamalai University, Annamalai Nagar Code Number: dv04038 Sir, Foreign body in the vagina is a common cause of vaginal discharge, which may be either purulent or hemorrhagic. This may result from ignorance, accident, malice, attempts at sexual stimulation or psychotic tendencies.[1] Young children tend to explore all orifices and may place a variety of small objects in the vagina.[2] A 3½-year-old girl was brought to the outpatient department by her grandmother, with a complaint of dysuria and foul smelling mucopurulent discharge from the vagina since 3 days. The child had lost her father 10 days ago. As there were many relatives at home on account of the recent bereavement, the grandmother was not sure of any sexual abuse. Local examination revealed congestion of the external genitalia and crusting on both labia majora. There was no ulceration. A thick, foul smelling, mucopurulent discharge was seen at the vulval introitus. Per rectal examination could not be performed as the child was uncooperative. The child was treated with cotrimoxazole and symptomatic therapy. The grandmother was advised about the need for relevant investigations and was instructed to keep a strict vigil on the child′s movements and the likelihood of sexual abuse by any adult member in the family or in the neighborhood. A week later, the mother of the child presented two "closed "safety pins claimed to have been recovered from the child′s external genitalia. According to her, one pin came out on its own, while the other had to be taken out. The baby was continued on antibiotics and by the end of the second week, she was asymptomatic. Fifteen days later, the child presented again with similar complaints. On local examination, the tip of a safety pin could be visualized in the vagina [Figure - 1]. Under aseptic conditions and after sedating the child, two safety pins could be extracted from the vagina [Figure - 2]. The child was treated with a second course of antibiotics. Whether the pins were inserted by the child herself or by another child or an adult could not be established. The mother was counseled about possible sexual abuse and the need for psychiatric consultation if the child was doing this on her own. Three months after this, no similar complaint has been reported. An extraordinary variety of foreign bodies may be found in the vagina, including safety pins, hair grips, pencils and small jam jars. The patient is often mentally retarded or a young child.[3] Children insert toys, sweets, hairpins, etc. into the vagina mainly out of curiosity. Small pieces of toilet paper that find their way into the vagina are most common.[4] Foreign bodies may be also inserted for various reasons, as articles of toilet and hygiene, by accident, as therapeutic agents to induce abortion or as contraceptive devices. The effect of the object varies with its nature and shape. Perforation, abrasion, pressure necrosis and local vaginitis result in ulceration of the vaginal walls. This can involve neighboring structures to cause urinary and fecal fistulae.[5] Ascending infection may lead to salpingitis and peritonitis. Rarely, neglected pessaries can cause severe ulceration of posterior fornix and later vaginal carcinoma.[3] The predominant symptom is an offensive blood stained discharge, as was observed in our patient. The foreign body must be removed, which may be easy, although in young children a narrow illuminated endoscope may be needed. The vaginal wall heals by itself after removal, as was observed in our case. The presence of vaginal foreign body may be an indication of sexual abuse. Though this is not always the case, the possibility should be kept in mind while examining any child with vulvovaginal symptoms.[6] In the present case, whether this was abuse by an adult or a childish prank by other children in the neighborhood or curiosity on the part of the child herself, is a question which still remains unanswered. REFERENCES
Copyright 2004 - Indian Journal of Dermatology, Venereology, Leprology The following images related to this document are available:Photo images[dv04038f1.jpg] [dv04038f2.jpg] |
| |||||||||

{kind=link}
{kind=link}