 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
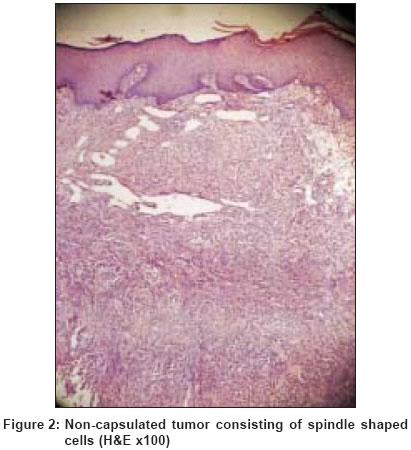
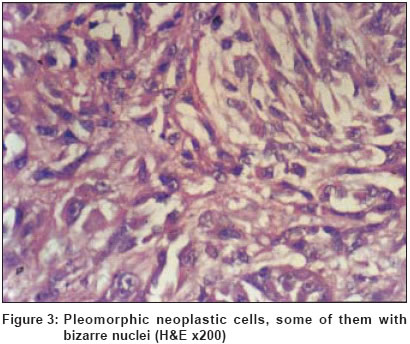
Indian Journal of Dermatology, Venereology, Leprology, Vol. 70, No. 2, March-April, 2004, pp. 139-141 Quiz Ulcerated nodule over the chest Jeevankumar B, Thappa Devinder Mohan , Shivaswamy KN, Jayanthi S Departments of Dermatology and STD, Jawaharlal Institute of Postgraduate Medical Education and Research (JIPMER), Pondicherry - 605006 Code Number: dv04045 A 25-year-old male agricultural laborer presented with a non-healing ulcerated nodule located on the upper chest, of three months′ duration. The lesion had started insidiously as a single pea-sized nodule. It progressively increased to achieve the present size and then subsequently ulcerated about a month ago. There was no history of preceding trauma or extrusion of bony chips from the lesion. Physical examination revealed a solitary ulcerated soft to firm nodule over the upper chest just medial to the right nipple [Figure - 1]. It measured 3 x 3 cm in size and exuded a serosanguineous discharge. There was no regional lymphadenopathy. Systemic examination revealed no abnormality. A chest X-ray was normal. Histopathological examination of the ulcerated nodule revealed a noncapsulated dense infiltrate of spindle shaped cells in the upper and mid-dermis [Figure - 2] and [Figure - 3]. Within this infiltrate, a few bizarre cells with pleomorphic hyperchromatic nuclei were also seen. Large bizarre multinucleated cells were arranged in a vague fascicular pattern. Scattered inflammatory cells and numerous small blood vessels were also present. What is your diagnosis? Diagnosis: Atypical fibroxanthoma. DISCUSSION Atypical fibroxanthoma (AFX) is a pleomorphic spindle cell tumor that usually occurs in the sun-damaged skin of the head and neck area of elderly individuals. Helwig[1] first introduced AFX as a diagnostic term in 1960, emphasizing its high pleomorphic histologic appearance, which contrasted with a generally benign course.[2] It has been earlier regarded as one of the ′pseudo-malignancies′ of the skin.[3] The etiology of AFX remains elusive.[2]-[4] Solar radiation probably represents a predisposing factor in the pathogenesis of this disease. This is supported by its common occurrence on actinically damaged skin. Other less well-documented factors include occupational and therapeutic irradiation. AFX has two forms of presentation.[2] In the commoner form, the disease affects the elderly individual. The tumor occurs on the exposed parts of the head and neck, particularly the nose, cheek and ear. In the less common form, the tumor occurs on the limbs and trunk of young persons. Grossly, these lesions are solitary nodules or ulcers usually measuring less than 2 cm in diameter. They may abut the epidermis causing pressure atrophy or ulceration.[2] Alternatively, a grenz zone of uninvolved dermis may be present. The tumor compresses the skin appendages laterally and extends into the subcutis. Because of reported metastases to the regional lymph nodes and lungs, AFX is now widely regarded as a low-grade malignant neoplasm related to malignant fibrous histiocytoma, which it resembles histologically.[4] It has a more favorable prognosis because of its small size and superficial location, whereas malignant fibrous histiocytoma, a pleomorphic sarcoma of middle and late adulthood, manifests in the subcutaneous tissue (superficial tumor) or entirely in the muscle (deep tumor) as circumscribed multilobulated masses, most commonly in the thigh and buttock, and carries a less favorable prognosis.[3], [4] Histologically, AFX resembles the pleomorphic form of malignant fibrous histiocytoma.[3] It is characterized by bizarre cells arranged in a haphazard or vague fascicular or rarely storiform pattern. The histological variants of AFX include spindle cell, clear cell, osteoid, osteoclastic, chondroid, pigmented and granular cell types.[3] The cells occasionally possess small deposits of neutral fat as well as PAS positive, diastase-resistant material, probably reflecting degenerative changes. Features that denote a more aggressive behavior include vascular invasion, deep tissue invasion, tumor necrosis and possibly impaired host immunity.[5],[6] If facilities are available, electron microcopy, immunoperoxidase studies for a1-antitrypsin, a1-antichymotrypsin, markers for vimentin and factor XIIIa may be done.[7] The histologic features of most cases of AFX are diagnostic.[4] In some cases, especially the less pleomorphic tumors, immunohistochemical staining is helpful in distinguishing AFX from other spindle cell neoplasms. AFX expresses vimentin and is non-reactive for cytokeratin, S-100 protein, and usually desmin, thereby excluding spindle cell squamous cell carcinoma, spindle cell melanoma, and most cases of leiomyosarcoma.[4] Other conditions sometimes mistaken for AFX include noduloulcerative basal cell carcinoma and osteoma cutis.[1]-[3],[8] Atypical fibroxanthoma is usually cured by simple excision.[8] REFERENCES
Copyright 2004 - Indian Journal of Dermatology, Venereology, Leprology The following images related to this document are available:Photo images[dv04045f2.jpg] [dv04045f1.jpg] [dv04045f3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}