 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
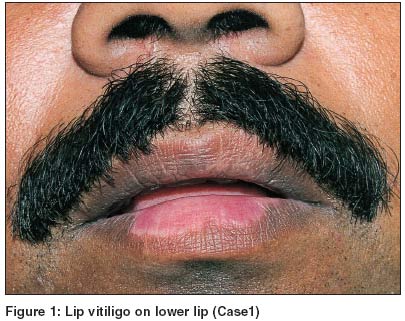
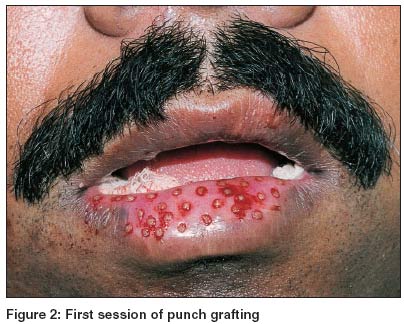
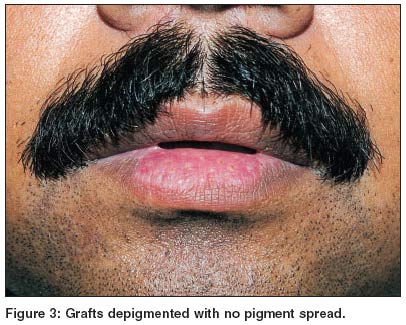
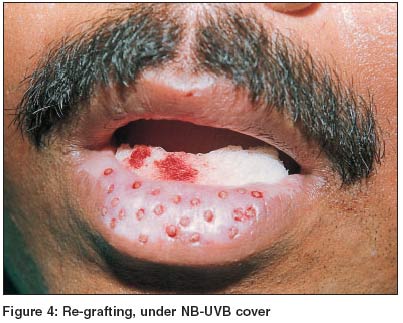
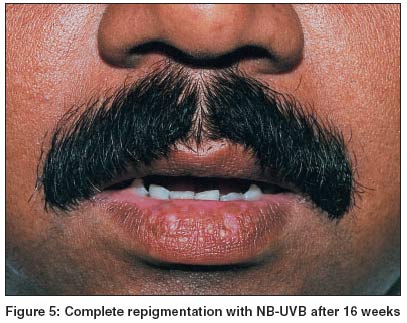
Indian Journal of Dermatology, Venereology, Leprology, Vol. 70, No. 3, May-June, 2004, pp. 156-158 Studies Inducing repigmentation by regrafting and phototherapy (311 nm) in punch grafting failure cases of lip vitiligo: A pilot study Lahiri Koushik , Malakar Subrata , Nilendu , Banerjee Uttam Pigmentary Disorder Unit, Rita Skin Foundation, GD-381, Sector III, Salt Lake, Kolkata - 700 106 Code Number: dv04050 ABSTRACT BACKGROUND: Punch grafting followed by PUVA/PUVASOL is an established mode of therapy in vitiligo including that on the lips. AIMS: To assess the efficacy of NB-UVB along with regrafting in patients in whom punch grafting had failed to evoke any response. METHODS: Five patients with stable and isolated lip vitiligo in whom punch grafting and PUVA had failed to produce pigmentation were treated by regrafting and subsequent NB-UVB (311 nm) phototherapy. RESULTS: Complete repigmentation was observed in three of the five cases after 16 weeks. In the remaining two, the results were mixed. CONCLUSIONS: Stable lip vitiligo usually responds very well to punch grafting and PUVA/PUVASOL. In patients who fail to respond to this treatment, complete repigmentation following regrafting and NB-UVB is an observation that needs to be explained.INTRODUCTION Lip vitiligo (LV) occurs either as an isolated condition or as an extension of vitiligo vulgaris. Owing to a complete lack of pigment cell reservoir in the lips, medical management often fails to repigment the achromic lip. In such cases punch grafting (PG) is considered to be the easiest, fastest and least expensive treatment modality even on the lips.[1] Punch grafting (PG) followed by PUVA/PUVASOL is an effective therapy.[2],[3],[4],[5] In the present study an attempt was made to explore the efficacy of narrow band-ultraviolet B (NB-UVB) phototherapy along with regrafting in patients of LV in whom punch grafting had failed to evoke any response. MATERIAL AND METHODS Regrafting was done at the insistence of one patient of LV in whom PG had failed [Figure - 1], [Figure - 2], [Figure - 3], [Figure - 4] and who was on NB (311 nm) phototherapy. The new grafts started showing spread of pigment and within 4 months his lip was completely repigmented [Figure - 5]. Inspired by this, we performed regrafting in another four patients with LV who had failed to respond to PG. None of them had a history of herpes simplex. All cases were stable for at least 6 months and lacked Koebner phenomenon. Test grafting was done in doubtful cases.PG was performed with 1.5 mm punches. The grafts were placed directly from the donor area (buttock or upper thigh) to the recipient area so as to speed up the procedure and lessen the chance of infection. Same sized punches were used for both the sites. If both the lips were involved, one lip was taken up for grafting at a time to avoid inconvenience to the patient. There were three layers of dressing from inside out: paraffin-embedded gauze (Gelonet ®), Surgipad ® and Micropore ®. The patients were advised to take a liquid diet for the first 24 hours, preferably with a straw. The dressings were removed on the 3rd or 5th post-operative day. Most of our patients were of skin types Fitzpatrick 4 and 5. All were put on NB phototherapy (311 nm) by a Speigel series 8 machine with Philips TL/01 311 nm lamps before and after PG. The dose was 8.41 mw/cm2. The minimal erythema dose (MED) was calculated; the average MED was 1261.5 mJ/cm2. A suberythemal dose of 1000 mJ/cm2 was used initially. It was increased by 10% to 20% per treatment. After 10 weeks (20 treatments) the increment rate was reduced to 2% to 5% up to a maximum of 2270 mJ/cm2. RESULTS A total of 66 grafts were placed on 5 individuals. The lower lip was grafted in 4 patients and both lips in 1. Repigmentation started within 16 days in one patient, and on the 19th and 20th day respectively in another two. In one patient no pigment spread was observed even 12 weeks after the second session. In the last patient pigment spread was very slow and unsatisfactory. Graft rejection was not noted in our patients. Transient cobblestoning was observed in one patient, but it subsided with time. The donor area healed with minimal scarring in all the cases. DISCUSSION The melanocytes are stimulated during photochemotherapy in vitiligo. They migrate from the hair follicle reservoir, spread centrifugally from the infundibulum to the basal cell layer and recolonize the epidermis with functional pigment cells. This does not occur on the lips as there are no hair follicles, explaining why medical management often results in a slow or poor response. Thus, transplantation of melanocytes by any of the surgical modalities is the most logical procedure in these cases. In our opinion, early treatment of LV by surgical methods speeds up the repigmentation and thereby avoids frustration both for the patients and doctors.[1] Amongst the various phototherapy options, NB-UVB therapy (311 nm) is effective and has a good safety profile.[6],[7],[8],[9],[10],[11] Stable LV usually responds well to punch grafting and PUVA/PUVASOL,[1] but herpes simplex induced lip leucoderma does not.[12],[13] The first session of PG failed to evoke any result in our patients of LV, but complete repigmentation occurred after regrafting and NB-UVB. Recently, perilesional and circulating melanocyte-specific cytotoxic CD8 cells have been identified and it was also found that UVB therapy promotes T-cell apoptosis.[14],[15] This theory may explain our observation of repigmentation after regrafting and NB-UVB therapy. To the best of our knowledge such an effort of regrafting followed by phototherapy (311 nm) in repigmenting failed cases of lip vitiligo was not attempted before. REFERENCES
Copyright 2004 - Indian Journal of Dermatology, Venereology, Leprology The following images related to this document are available:Photo images[dv04050f2.jpg] [dv04050f3.jpg] [dv04050f5.jpg] [dv04050f4.jpg] [dv04050f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}