 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
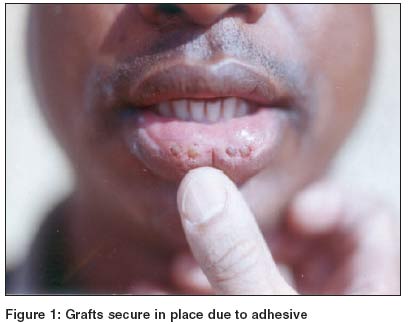
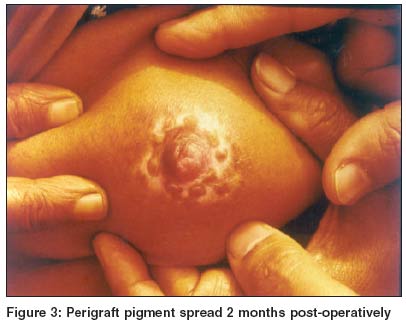
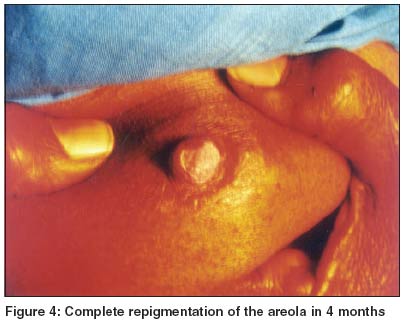
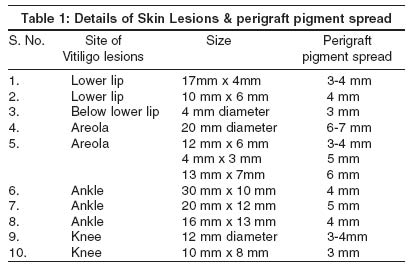
Indian Journal of Dermatology, Venereology, Leprology, Vol. 70, No. 3, May-June, 2004, pp. 159-161 Studies Use of tissue glue for punch grafting in vitiligo - A preliminary report Ghorpade Ashok Department of Dermatology, Venereology and Leprosy, JLN Hospital and Research Centre, Bhilai Steel Plant, Bhilai (CS) Code Number: dv04051 ABSTRACT BACKGROUND: Minipunch grafting has been successfully used for the treatment of stable vitiligo since several years. Post-operative immobilization at certain sites such as lips, areola & infralabial folds and joints is not easy to achieve. Putting stay sutures on the lips and areolae is difficult. Grafting over the joints may require hospitalization to ensure proper immobilization, and may discourage some patients. AIM: To study the efficacy of a tissue glue for immobilization of donor grafts at the above sites during minipunch grafting. METHODS: Ten cases with stable vitiligo over the lips, areolae, below the lower lip, and over different joints had tissue glue applied to the edges between the donor grafts and the recipient wells, after the grafting. RESULTS: The grafts adhered firmly within a minute and there was no need for a cumbersome dressing. Over the lips, the patients could resume talking and drinking fluids immediately. CONCLUSION: The glue was very helpful for immobilizing the grafts at these difficult sites.INTRODUCTION Cyanoacrylates, which are surgical adhesives, are being increasingly used as an alternative to sutures in various surgical specialties to provide wound closure. They are as effective as sutures in low tension lacerations, and are useful in emergency rooms and in the first aid of patients where wound closure is required but sutures are not warranted. They have been used during hair transplantation,[1] split thickness skin grafting,[2] for closing cerebrospinal fluid leak,[3] punctal occlusion[4] and full thickness skin grafting.[5] They have been found helpful in children as an alternative to sutures, eliminating the need for an injection of local anesthetic. The purpose of the study was to find its effectiveness in providing quick and effective immobilization of donor grafts used for vitiligo at some difficult sites. METHODS This preliminary work was carried out on ten cases of vitiligo where the lesions had been stable for at least a year. Eight patients were males and 2 females. Their age varied between 18 and 65 years. Most (eight) patients were between 18 and 35 years of age. Two patients had vitiligo on the lower lip, one below the lower lip, three over the ankle and two over the knee joints. There were two females (18 years and 55 years of age) with stable vitiligo localized to the areolar region. In 8 patients, grafts were taken from the anterior aspect of the thighs, while for the lips, the donor site was the retroauricular region. The punches used for donor grafts and recipient wells in all patients were of the same size and varied between 2.5 mm and 4 mm in diameter. Lip lesions required 4 grafts each, lesions below the lip two grafts, ankle and knee joint lesions between 5-15 grafts and the areolar region 6-11 grafts. After following the standard procedure for minipunch grafting, and keeping the grafts in recipient wells, the area was dried. A single use plastic ampoule containing the liquid tissue glue [n-butylcyanocrylate (tiglu)] was cut at the nose, where the sterile needle provided was fixed immediately. The ampoule was then inverted and pressed lightly to squeeze out a tiny droplet of the adhesive, which was carefully applied in between the donor grafts and the recipient wells, leaving a gap between two applications. If the requirement of the adhesive was found to be less than even a tiny droplet, a little modification was tried. The tiny droplet expressed from the needle tip was broken further into even smaller droplets by taking it on another sterile needle tip, and applied only at four points, at 12, 3, 6 and 9 o'clock positions between the edges of the donor grafts and the recipient wells. This modification was to avoid excess application of the adhesive to the surrounding area, which may stick to the graft or injure the normal skin and may interfere with healing. Thick applications do not enhance bonding and tend to crack and loosen prematurely. The adhesion between the graft and the recipient wells started within 10 seconds and was complete within 1 minute of application [Figure - 1]. No dressing or immobilization was required in any patient. Patients with grafts over the lips were allowed to take liquids orally immediately after the procedure. Topical antibiotics were not used since they may lead to sloughing. All the patients received oral erythromycin 250 mg 6 hourly for 7 days after grafting. The glue is biodegradable in about 7-14 days. The patients were followed up after 7 days, and were put on PUVASOL therapy after 2 weeks. RESULTS In all the cases the grafts took up very well. The perigraft pigmentation was good in all the cases and resulted in complete repigmentation in 4-5 months. [Figure - 2], [Figure - 3], [Figure - 4]. The size of lesions and the perigraft pigment spread in each patient is shown in [Table - 1]. None of them developed any complications during the follow up of 2 years. DISCUSSION The glue was found quite useful as it was easy to apply, and eliminated the need for immobilization, admission, post operative dressing and frequent follow up. There were no complications. The single use ampoule, having 0.25 ml of the glue, costs less than Rs. 200, and seems to be cost effective, considering the cumbersome, traumatic and time consuming alternative of stay sutures and admission. To the best of my knowledge, the use of cyanoacrylate tissue glue at these sites in vitiligo surgery has not been reported earlier. The glue may also be helpful in areas that are difficult to suture, like the genitalia, groin, eyelids, palms, and fingertips. This is a preliminary report, where the results seem to be quite encouraging. Tissue glues have been used on traumatic lacerations,[6] and have been found to be as good as or even better than sutures during atheletic injuries.[7] Delayed depigmentation and carcinogenicity have been mentioned after the use of tissue glue, and further large scale studies on the use of tissue glue may help in throwing light on its advantages and or disadvantages at a few special sites in vitiligo surgery. REFERENCES
Copyright 2004 - Indian Journal of Dermatology, Venereology, Leprology The following images related to this document are available:Photo images[dv04051f3.jpg] [dv04051f2.jpg] [dv04051f4.jpg] [dv04051t1.jpg] [dv04051f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}