 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
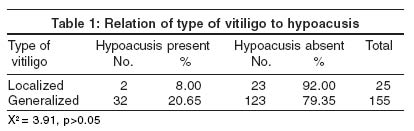
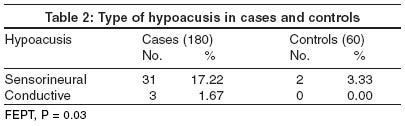
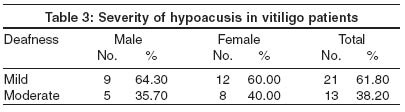
Indian Journal of Dermatology, Venereology, Leprology, Vol. 70, No. 3, May-June, 2004, pp. 162-164 Studies Hypoacusis in vitiligo Sharma Lata , Bhawan R, Jain RK Departments of Dermatology and Venereology, Institute of Medical Sciences, Banaras Hindu University, Varanasi Code Number: dv04052 ABSTRACT BACKGROUND: Vitiligo affects melanocytes in the skin. Since melanocytes are present in other organs as well, it is plausible that they may be similarly affected. METHODS: A comparative study of audiological functions was carried out in 180 patients of vitiligo and 60 non-vitiligo controls in the age group of 5-40 years. RESULTS: In vitiligo patients sensorineural hypoacusis of mild degree was found in 18, moderate in 13 and mild conductive hypoacusis in 3. In controls sensorineural hypoacusis of mild degree was found in only 2 cases. CONCLUSION: The difference between the two groups was statistically significant. Vitiligo patients have a higher prevalence of sensorineural hypoacusis.INTRODUCTION Vitiligo is an ancient pigmentary disorder of the skin, but the finding of altered cutaneous functions is recent.[1],[2],[3] Ocular and audiologic abnormalities have also been observed because these organs are morphologically and developmentally related to the skin.[4],[5] There is a difference in noise induced hypoacusis in white and black skinned individual because of a difference in the quantity of pigment cells present in the inner ear.[6],[7] Audiological functions have been studied in vitiligo by Tosti et al[5] in Italy, but since there was no comparable study from India, we planned to compare the audiological functions in patients of vitiligo and controls in our country. METHODS One hundred and eighty patients of vitiligo and 60 non-vitiligo controls in the age group of 5-40 years were enrolled from the Skin & V.D. Out Patient Department. Patients exposed to factors known to produce hypoacusis such as noise, drugs, infections, and injuries to the ear were excluded. Patients suffering from metabolic, vascular or autoimmune diseases or any systemic disease like diabetes, hypertension or tuberculosis were excluded. The duration, type and distribution of vitiligo along with details of treatment received were noted in a proforma. An otoscopic examination for both ears was done and the results of tuning for Rinne's and Weber's tests and absolute bone conduction were recorded. Audiometry was done by pure tone audiometer (Arphi audiometer Mark-3) in a silent cabin. Air conduction measurements were done for test frequencies 250 Hz to 4 KHz and bone conduction from 250 Hz to 4 KHz for both ears. The scale of hearing impairment was assessed according to the 1964 International Standard Organization hearing threshold parameters, i.e. normal: inability to hear at minus 10 to 20 db, mild deafness: inability to hear at 27-40 db, moderate deafness: inability to hear at 41-55 db. Patients were also investigated for blood hemoglobin and sugar levels, total and differential leukocyte counts, erythrocyte sedimentation rate, and urine for albumin and microscopic examination. For statistical analysis, Chi-square and Fisher's exact probability tests (FEPT) were applied RESULTS One hundred and three females and 77 males suffering from vitiligo were studied. Of these, 117 were in the age group of 5-22 years and 63 in 23-40 years. The duration of vitiligo was less than 5 years in 96 and more than 5 years in 84 cases. One hundred and fifty five cases had the generalized type of vitiligo and 25 had the localized type. Patients did not complain of deafness but on audiological examination hypoacusis was found in 34 patients (18.89%) and in 2 non-vitiligo controls (3.33%), which was statistically significant (X2 = 7.36, p<0.01). Out of these, 23 patients gave a history of taking treatment for vitiligo while 11 cases were untreated. There were 14 males (18.18%) and 20 females (19.42%) manifesting hypoacusis, 20 in the 5-22 years age group and 14 in the 23-40 years age group. There were 116 students, 7 house workers, 6 farmers, 3 businessmen and 2 service class patients. In non-vitiligo controls, there was 1 female student and 1 housewife, the former presented for acne and the latter for melasma. Hypoacusis was not affected by age, sex, occupation and therapy of vitiligo. Deafness was present in 18 out of 96 patients (18.75%) having vitiligo for less than 5 years and 16 out of 84 (19.05%) for more than 5 years (X2 = 0.002, p<0.05). This shows that deafness was not related to the duration of vitiligo. Thirty two cases of the generalized type of vitiligo and 2 of the localized type had hypoacusis, which was statistically significant (X2 = 3.91, p>0.05) [Table - 1]. Hypoacusis was of the sensorineural type in 31 (17.22%) patients and 2 controls (3.33%) and of the conductive type in 3 patients (1.67%) [Table - 2]. Hypoacusis was mild in 21 patients (61.80%), including 3 cases of the conductive type and 18 of the sensorineural type, and moderate in 13. Hypoacusis in 2 controls was of the mild sensorineural type [Table - 3]. DISCUSSION Vitiligo is a disorder of melanocytes. Melanocytes arise from the neural crest in embryonic life. The embryonic ectoderm also originates from the margins of the neural plate which forms the tubular central nervous system. The inner ear develops from the hind brain.[6] Thus both melanocytes and the inner ear are ectodermal in origin.[9] The inner ear is the organ of hearing. It consists of the bony and membranous labyrinth. The bony labyrinth contains the cochlea. The auditory receptors or hair cells are present in the organ of corti which is located on the basilar membrane of the cochlea. This organ extends from the apex to the base of the cochlea and consequently has a spiral shape. Melanocytes are present in this region.[6] The melanocytes in the inner ear are thought to prevent damage to the hair cells due to environmental ototoxic agents. Therefore alteration in pigment cells might result in deafness.[10] The results show that out of 180 patients of vitiligo, 34 (18.89%) had hypoacusis as compared to 2 patients (3.33%) out of 60 in the control group (X2 = 7.36, p<0.01), which was statistically significant. It was of the sensorineural type in 31 patients and of a mild degree in most of them. The results of the study carried out by Tosti et al[5] in Italy showed that 8 out of 50 patients of vitiligo (16%) had sensorineural hypoacusis and are similar to the data obtained in this study. Hence differences in the skin color in patients of different countries may not affect the incidence of audiological abnormalities in vitiligo patients. The number of patients with deafness was significantly more in the generalized type of vitiligo than in the localized type (X2 = 3.91, p>0.05). This indicates that the effect on melanocytes was generalized. The deafness was not severe or total as the vitiligo was also not involving the whole body. In a larger audiological study it may be possible to predict whether the vitiligo in patients is going to be localized or generalized. Deafness was not related to duration, progress and psoralen therapy. This is difficult to explain by the theory of destruction of melanocytes in vitiligo by the autoimmune mechanism. From the demonstrable alterations in the cutaneous physiology of vitiligo lesions,[2] like increased blister resorption time, increased bleeding time, decreased sweat response and decreased patch test response and with the recognized association of ocular and auditory abnormalities,[4] it is reasonable to consider that vitiligo is more than a skin disease. REFERENCES
Copyright 2004 - Indian Journal of Dermatology, Venereology, Leprology The following images related to this document are available:Photo images[dv04052t2.jpg] [dv04052t1.jpg] [dv04052t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}