 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
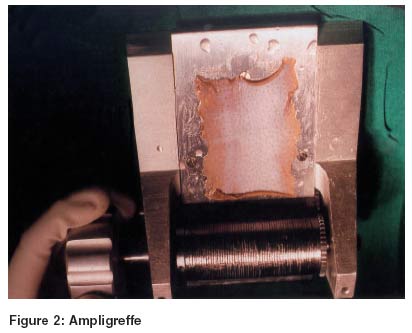
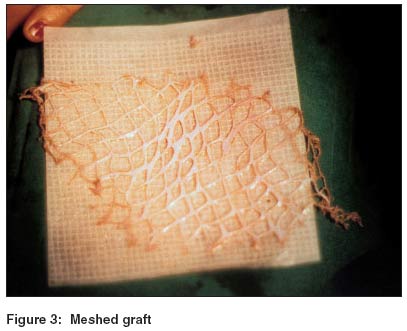
Indian Journal of Dermatology, Venereology, Leprology, Vol. 70, No. 3, May-June, 2004, pp. 165-167 Case Report Meshed split skin graft for extensive vitiligo Srinivas CR, Rai Reena , Kumar PUday Department of Dermatology, PSG Institute of Medical Sciences and Research, Peelamedu, Coimbatore - 641 004 Code Number: dv04053 ABSTRACT A 30 year old female presented with generalized stable vitiligo involving large areas of the body. Since large areas were to be treated it was decided to do meshed split skin graft. A phototoxic blister over recipient site was induced by applying 8 MOP solution followed by exposure to UVA. The split skin graft was harvested from donor area by Padgett dermatome which was meshed by an ampligreffe to increase the size of the graft by 4 times. Significant pigmentation of the depigmented skin was seen after 5 months. This procedure helps to cover large recipient areas, when pigmented donor skin is limited with minimal risk of scarring. Phototoxic blister enables easy separation of epidermis thus saving time required for dermabrasion from recipient site. INTRODUCTION Vitiligo is a heritable disease with melanocytopenia. The modalities of treatment include medical and surgical methods. We describe a patient with generalized stable vitiligo unresponsive to medical treatment who showed significant pigmentation following grafting of the large recipient areas with a meshed split skin graft. CASE REPORT A 30-year-old female presented with generalized stable vitiligo involving large areas of her body since 5 years [Figure - 1]. She received 60 mg prednisolone once a week and PUVA therapy twice a week for 1 year. Punch grafting was done for her eyelids, dorsum of hands and feet, and PUVA therapy was continued. Since the patient had generalized stable vitiligo with large recipient areas we used meshed split skin grafting.On the vitiliginous areas 0.075% of 8-methoxypsoralen was applied and after 10 minutes the affected part was exposed to 10 J/cm2 of UVA in PUVA full body unit (V Care Ltd., India) for two consecutive days before surgery. On the day of the surgery the vitiliginous skin was erythematous with blisters over few areas. Under general anesthesia, a 0.01 mm thickness graft was obtained from the anterolateral aspect of the thigh using a Padgett dermatome (Collin, France). The dermatome was held at a 45° angle and the graft was cut rapidly. The graft, which automatically folds itself into the pocket of the dermatome, was severed by lifting the instrument away from the donor site. The grafts were transferred to an ampligreffe (Collin, France) [Figure - 2]. The ampligreffe contains a slightly inclined metal plate over which the graft was placed with the dermis facing upwards. One end of the graft was gently inserted between the spiral barrels of the ampligreffe. The handle of the ampligreffe was then rotated. This resulted in the graft passing between the two barrels which formed a diamond shaped mesh in the graft. This transformed the graft into a mesh four times the size of the original graft. The meshed skin with the dermal surface facing upward was spread on ©Sofratulle [Figure - 3]. The erythematous and blistered vitiliginous skin was rubbed vigorously with a saline-soaked gauze piece held between the thumb and index fingers to remove the epidermis. Areas of epidermis not removed by this procedure were dermabraded using a Kurtins stainless steel wire planing brush (Robbin). The Sofratulle with meshed skin was placed on the dermabraded area. The grafts were kept in position by bandaging using saline-soaked gauze. A 4" crepe bandage was used to apply firm pressure. The dressing was changed after 4 days and removed after 7 days and the patient subjected to PUVA therapy twice a week. Repigmentation at the recipient site was noticed after one year [Figure - 4]. The donor site showed post-inflammatory hyperpigmentation but no scarring. DISCUSSION The various medical modalities of treatment for vitiligo include PUVA therapy, UVB therapy and corticosteroids.[1] Patients during their course of medical treatment can be surgically treated for rapid repigmentation. The surgical treatments include blister roof grafting,[2] punch grafting followed by PUVA therapy,[3] melanocyte culture and transplantation,[4] split skin grafting[5] and dermabrasion.[6] Blister roof grafting yields a limited amount of skin. Punch grafting, though effective, is time consuming and the area treated is limited by the amount of local anesthesia which can be used.[7] A split thickness graft covers the recipient area in a 1:1 ratio thus necessitating large grafts from the donor area. By using an ampligreffe and increasing the size of the graft by 4 times, we were able to cover large areas with smaller grafts from donor areas. The advantage of the ampligreffe is that there is no tissue damage and it adapts to a wrinkled or irregular surface. Dermabrasion is a time consuming procedure and it is difficult to achieve a uniform depth. Topical psoralen followed by UVA in a higher dose prior to treatment leads to separation of the epidermis from the dermis. The epidermis can be rapidly removed by using saline-soaked gauze.[8] The authors have been using this technique for the past 10 years with good results and no long term complications. The above procedure enabled us to rapidly harvest the graft, quickly dermabrade the recipient area and also cover larger recipient areas. There is no risk of scarring by inducing a phototoxic blister in the recipient site since there is no involvement of the deeper dermis. There is minimal risk of scarring at the donor site as very thin grafts are taken. The irregularity of pigmentation which is noticed following all surgical procedures is likely to improve in due course. Even if minimal irregularity persists patients prefer this to the depigmentation. We recommend this procedure when large areas have to be grafted and pigmented donor skin is limited. REFERENCES
Copyright 2004 - Indian Journal of Dermatology, Venereology, Leprology The following images related to this document are available:Photo images[dv04053f1.jpg] [dv04053f4.jpg] [dv04053f3.jpg] [dv04053f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}