 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
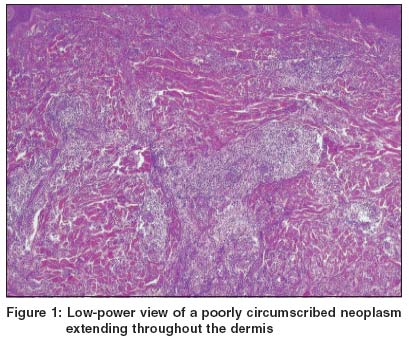
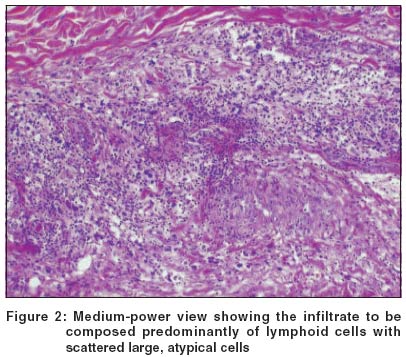
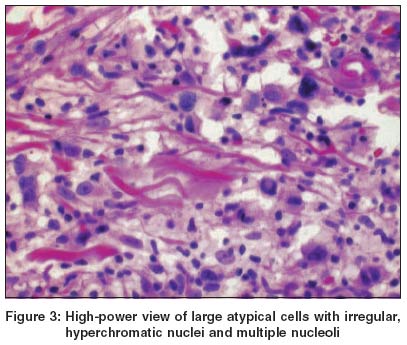
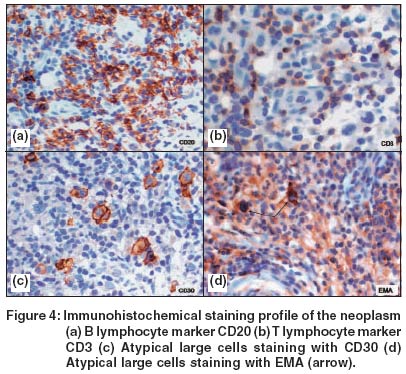
Indian Journal of Dermatology, Venereology, Leprology, Vol. 70, No. 3, May-June, 2004, pp. 168-171 Case Report Cutaneous anaplastic large cell lymphoma - A case report Mahalingam Meera , Bhawan J Quest Diagnostics Incorporated, Cambridge, MA Code Number: dv04054 ABSTRACT Cutaneous involvement in anaplastic large cell lymphoma may be in the form of primary cutaneous disease (primary cutaneous anaplastic large cell lymphoma) or secondary to involvement by systemic disease (systemic anaplastic large cell lymphoma). This case report, an example of the latter, describes a solitary cutaneous lesion as the first evidence of disseminated neoplastic disease. The histology of the lesion was identical to its primary cutaneous counterpart.INTRODUCTION The CD30 molecule, a member of the tumor necrosis factor (TNF) receptor superfamily, is found on the cell membrane and in the Golgi region of cells.[1] The discovery of Ki-1, an antibody directed against the CD30 molecule, led to the recognition of a novel category of lymphomas known as anaplastic large cell lymphoma (ALCL).[2] Defining features of ALCL were the cohesive proliferation of large, pleomorphic blast-like cells all expressing CD30.[2] Besides the systemic form of ALCL, a primary cutaneous form of ALCL (primary cutaneous ALCL), encompassing approximately 9% of all cutaneous lymphomas, has also been since described.[3],[4],[5] Primary cutaneous ALCL has been shown to have a more favorable prognosis than systemic ALCL.[6] This report describes a solitary cutaneous nodule as the first evidence of metastatic disease in a patient with systemic ALCL previously treated successfully. Histologic features were identical to its primary cutaneous counterpart. This case is another good example of metachronous metastases, with the tumor developing years after the diagnosis and treatment of the primary malignancy.[7],[8] CASE REPORT A 51-year-old female presented with a 2 cm tan-colored nodule on the right leg. Clinical diagnosis was that of dermatofibroma. Although no clinical history was provided initially, a review of the patient's chart revealed a history of nodal-based CD30 positive large cell lymphoma (systemic ALCL) - diagnosed and treated successfully two years prior to the current presentation. Microscopic examination revealed a poorly circumscribed neoplasm composed of lymphoid cells extending throughout the dermis [Figure - 1]. Scattered, atypical, large cells with irregular, hyperchromatic nuclei, multiple nucleoli and abundant cytoplasm were noted [Figure - 2], [Figure - 3]. Immunohistochemical stains revealed the cellular infiltrate to be diffusely and strongly positive for CD45 (Leukocyte Common Antigen/LCA), with admixed B (CD20 positive, [Figure - 4]a and T (CD3 positive, [Figure - 4]b lymphocytes. The atypical, large cells were diffusely and strongly positive for CD30 [Figure - 4]c with rare cells showing positivity for EMA (Epithelial Membrane Antigen [Figure - 4]d. DISCUSSION Cutaneous CD30 positive lymphoproliferative disorders may be primary (primary cutaneous ALCL) or secondary (systemic ALCL).[9],[10] Despite the unifying histologic feature of the presence of large, atypical cells expressing CD30, prognostic differences exist between these groups.[6],[10],[11] In one study with a median follow-up of approximately two years, spontaneous regression of skin lesions was observed in 44% of patients with primary cutaneous ALCL compared to 20% of patients with cutaneous involvement secondary to systemic ALCL.[9] Therefore, despite the overlap in histologic and immunophenotypic features, management of patients with cutaneous involvement secondary to systemic ALCL typically tends to be more aggressive.[11] The histopathologic differentiation between these two groups is of obvious relevance to patient management obviating the need to wait for the 6-month interval without extracutaneous spread - a criteria essential for the diagnosis of any primary cutaneous lymphoma. The histologic clue to the diagnosis of ALCL, cutaneous or systemic, is the presence of large lymphoid cells, seen in the case presented and also known as "hallmark cells", with embryonal nuclei, multiple prominent eosinophilic nucleoli and abundant cytoplasm. Given that the similarity in histology makes it difficult, if not impossible, to differentiate primary cutaneous ALCL from cutaneous involvement secondary to systemic ALCL on histopathologic grounds alone, several histologic and immunologic parameters have been studied in an attempt to define those that are of use in enabling differentiation between the two.[5],[6],[11] The two that are frequently cited to be of use are EMA and the chimeric protein p80 or nucleophosphomin-anaplastic lymphoma kinase (NPM-ALK).[6],[12] The latter is a consequence of the balanced t(2;5)(p23;q35) translocation associated with ALCL.[13] The expression of EMA, a finding corroborated in the case presented, is found to be more frequent in cutaneous involvement secondary to systemic ALCL. Although EMA has been primarily considered as an indicator of large cell activation, in one study EMA expression was found not to statistically correlate with prognosis.[6] Regarding expression of the chimeric protein NPM-ALK, conflicting data exist.[6],[12],[14],[15] While one study shows it to be present in both primary cutaneous and systemic ALCL, there are several others indicating its presence only in systemic ALCL. Although this discrepancy may be a function of the different methods (Southern blot vs. RT-PCR vs. FISH) used, these data emphasize the need for a standardized method for detection of the chimeric protein before using its expression as an adjunct tool to discriminate between these two entities. The presence of the chimeric protein, like EMA, does not appear to be a prognostic factor for primary cutaneous or systemic ALCL.[6] Clinical follow-up of the patient in the case presented included staging studies to exclude evidence of metastatic disease elsewhere. The treatment regimen of the patient comprised local radiation in fractionated doses and combination chemotherapy. Eighteen months post-treatment, the patient is well with no evidence of new lesions and negative CT scans of the chest, abdomen and pelvis, negative gallium and bone scans, and a negative bone marrow biopsy. As with most lymphomas metastasizing to the skin, this case is another example of the difficulties encountered by a practicing dermatopathologist in making a diagnosis in the absence of pertinent clinical history. Also, while routine light microscopy is certainly helpful in making a preliminary diagnosis, this case highlights the utility of immunohistochemical stains in making a definitive diagnosis, and therefore, in directing the appropriate early management of patients with ALCL. There is growing evidence for a potential role of the CD30 molecule in clinical use and therapy.[1] It has been shown that survival of mice bearing xenografts of human CD30 positive ALCL has been prolonged when they are treated with anti-CD30 immunotoxin.[16] Given that the chimeric protein NPM-ALK binds to the intracellular domain of the CD30 molecule, a speculative, yet scientific, hypothesis is that immunotherapy using anti-CD30 monoclonal antibodies may be the obvious way to treat categories of ALCL with poor prognosis such as the one presented in this case report.[17] REFERENCES
Copyright 2004 - Indian Journal of Dermatology, Venereology, Leprology The following images related to this document are available:Photo images[dv04054f3.jpg] [dv04054f2.jpg] [dv04054f1.jpg] [dv04054f4.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}